Download
1 / 42
530 likes | 3.7k Views
Peripheral Joint Mobilization -- Shoulder Joints. Huei-Ming Chai, PT PhD School of Physical Therapy National Taiwan University, Taipei, Taiwan June 23, 2008. Manual Therapy. Joint mobilization for restoration of joint alignment or joint mobility osteokinematics (physiological movement)

E N D
Peripheral Joint Mobilization-- Shoulder Joints Huei-Ming Chai, PT PhD School of Physical Therapy National Taiwan University, Taipei, Taiwan June 23, 2008
Manual Therapy • Joint mobilization for restoration of joint alignment or joint mobility • osteokinematics (physiological movement) • arthrokinematics (accessory movement) • Mulligan’s techniques: SNAG, MWM • Soft tissue mobilization for establishment of muscular balance (neuromuscular therapy) • PNF stretch • muscle energy technique • Sweden massage • deep friction massage • myofascial release • connective tissue massage • nerve mobilization • Chinese massage
Mobilization vs. Manipulation • mobilization: repetitive passive movement of varying amplitudes of low velocity applied at different parts of the range depending on the effects desired • manipulation: a high-velocity thrust of small amplitude performed at the limit of available movement
Rationales of joint mobilization • To relieve pain and muscle guarding increasing proprioceptive input to the spinal cord so as to inhibit ongoing nociceptive input to anterior horn cells and central receiving area • To restore accessory movement (joint play)
Concave-Convex Rule convex on concave concave on convex
Treatment Plane • treatment plane is the plane that parallel to the articular surface of the concave component of the joint to be treated • Kaltenborn FM: direction of mobilization define by treatment plane • Mulligan B: always parallel or perpendicular to treatment plane only
Closed-Packed Position • The joint surface becomes maximally congruent. • The joint capsule and major ligaments become twisted, causing joint surface to approximate. • The joint become locked so that no further movement is possible in that direction.
Position of Joint • appropriate for the stage of the joint problem and the skill of the therapist: • resting position: for an acute problem or an inexperienced therapist • other starting position toward motion barrier: for a skilled therapist in non-acute condition
Hand placement • fixation hand • stabilization of the joint component to be fixed • mobilizing hand • placing as close to the joint as possible
IV III II V I Range: initial limited full Techniques (I) • direction • distraction • gliding • amplitude • depending on pain, muscle guarding or degree of limitation • Maitland's grades
Techniques (II) • velocity • slow stretch for capsular or ligamentous tightness or adhesion: application with rhythm, slow speed, and the slack position • fast oscillation (rhythm: 2-3 cycles per second) for relieving of pain and muscle guarding in the • acute conditions as a treatment • chronic conditions to prepare for more vigorous stretching or to promote more relaxation of muscles controlling the joint
No Pain At All pain muscle spam vessel constriction nociceptive stimulation accumulation of metabolites
Indications (I) • used in the joints with restriction of joint play that cause pain or restriction of physiological motion, especially in the cases due to capsular or ligamentous tightness or adhesion • For gentle mobilization carried out in the pain-free range • severe pain • spasm increased after testing • presence of neurological deficit • pain disturbing sleeping • For more vigorous mobilization • joint irritability minimal with muscle guarding on movement • mobility testing limited but does not aggravate pain • limitation of motion by tension of tissues rather than pain • no neurological deficit
Indications (II) • For manipulation • used as a progression from vigorous mobilization that has not produced the maximum improvement of signs and symptoms considered possible • used as a primary treatment in joints with no articular inflammatory signs and the restricted joint has been identified through mobility testing • used in joints with minimal pain that appears only at the end of the range
Patient Response to Joint Mobilization • improved after treatment continue treatment until symptoms are subside • exacerbated for hours after treatment but improved later continue but decrease dosage • exacerbated immediately after treatment • reassess patient’s condition • gentle traction of the treated segment • documentation of all physical findings • stationary after 3-5 treatments re-evaluate patient’s condition
Absolute Contraindications • bacterial infection: • cellulitis • neoplasm with metastasis to bone: • malignancy or benign tumor (cancer) • recent fracture: psudoarthrosis • bone disease: Osteogenesis Imperfecta • potential destruction of ligaments or capsule: RA or dysplasia of odontoid process
odontoid process transverse ligament
Relative Contraindications • joint effusion • in the status of acute inflammation • degenerative joint disease in acute stage or bony block • marked rheumatoid arthritis • osteoporosis • internal derangement • general debilitation • pregnancy • hypermobility in mobility testing • moderate to severe deformities • psychological changes • neurosis • hysteria • depression
neutral rotation to left Relative Contraindications • for spinal mobilization • vertebral artery insufficiency • ligament instability
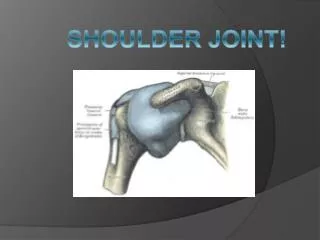
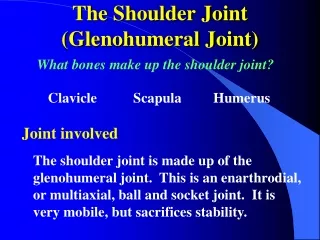
Mobilization to the Shoulder Joint • Glenohumeral joint • Thoracoscapular articulation • Sternoclavicular joint • Acromioclavicular joint
Glenohumeral Joint (GHJ) • convex on cave joint • proximal component: concave glenoid cavity • distal component: convex humeral head • joint type: ball and socket • DOF = 3 • flexion/ extension: posterior/ anterior glide • abduction/ adduction: inferior/ superior glide • external/ internal rotation: anterior/ posterior glide • Note: retroversion of the humeral head about 30º posterior to the frontal axis of the elbow joint (scapular plane)
Glenohumeral Joint (cont’d) • neutral position: anatomic position • resting position: 70 of shoulder abduction and 30 of flexion (horizontal adduction) • closed packed position: 90 of shoulder abduction and full external rotation
Basic Mobilization Techniques • distraction: anterolateral • inferior glide: inferolateral • posterior glide: posterolateral • anterior glide: anteromedial
Distraction of GHJ force direction: anterolateral
Inferior Glide of GHJ force direction: inferolateral
Posterior Glide of GHJ force direction: posterolateral
Anterior Glide of GHJ force direction: anteromedial
Advanced Mobilization Techniques • inferior glide with distraction • inferior glide with shoulder internal rotation • inferior glide in sitting position • posterior glide in sitting position
Inferior Glide of GHJ with Distraction force direction: inferolateral
Inferior Glide of GHJ with IR force direction: inferolateral
Posterior Glide of GHJ in Sitting force direction: posterolateral
Mobilization to the Shoulder Joint • Glenohumeral joint • Scapulothoracic articulation • Sternoclavicular joint • Acromioclavicular joint
Scapulothoracic Articulation (STA) • concave on convex • proximal component:convex rib cage • distal component:concave anterior surface of the scapula • motion: results of motions occurring at STJ and ACJ • scapular elevation/ depression • scapular abduction/ adduction • scapular upward/downward rotation • DOF = 3
Elevation of Scapula force direction: superior
Depression of Scapula force direction: inferior
Protraction/ Retraction of Scapula force direction: lateral
Mobilization to the Shoulder Joint • Glenohumeral joint • Scapulothoracic articulation • Sternoclavicular joint • Acromioclavicular joint
elevation depression P retraction posterior rotation A protraction Characteristics of SC Joint • proximal component -- sternum • saddle-shaped sternal manubrium • distal component -- clavicle • saddle-shaped medial end of clavicle • joint type: saddle joint • degree of freedom = 3 • motions
Mobilization to the Shoulder Joint • Glenohumeral joint • Scapulothoracic articulation • Sternoclavicular joint • Acromioclavicular joint
Acromioclavicular Joint • proximal component:convex lateral end of the clavicle • distal component:concave acromion process of the scapula • joint type:nearly plane joint • motion:shoulder girdle motion • scapular winging • scapular tipping • scapular upward/downward rotation • DOF = 3
物理治療師是您的好伙伴 柴惠敏 hmchai@ntu.edu.tw http://www.taiwanpt.net 謝謝您耐心聽講