Selective COX-2 Inhibitors
490 likes | 1.14k Views
Selective COX-2 Inhibitors. Pharmacology of Selective COX-2 Inhibitors (COXIBs). Discovery in early 1990: cyclo-oxygenase (COX) existed in 2 distinct isoforms While COX-1 and COX-2 are structurally similar COX-2 contains a side pocket. Pharmacology of Selective COX-2 Inhibitors (COXIBs).

Selective COX-2 Inhibitors
E N D
Presentation Transcript
Pharmacology of Selective COX-2 Inhibitors (COXIBs) • Discovery in early 1990: cyclo-oxygenase (COX) existed in 2 distinct isoforms • While COX-1 and COX-2 are structurally similar • COX-2 contains a side pocket
Pharmacology of Selective COX-2 Inhibitors (COXIBs) • Ratio of affinities to COX-1 and COX-2 determines how “selective” a compound is • NSAIDs inhibit COX-1 and COX-2 with different ratios • Differences in selectivity lead to some variability in • Clinical action • Safety profiles
Cyclo-oxygenase I (COX-1) • Constitutive enzyme • “House keeping” enzyme • Expresses ubiquitously • Mediates physiological responses
Cyclo-oxygenase I (COX-1) • Only isoenzyme found in platelets • Thromboxane A2 (TXA2) formation • Also plays a role in • Protection of GI mucosa • Renal hemodynamics • Platelet thrombogenesis
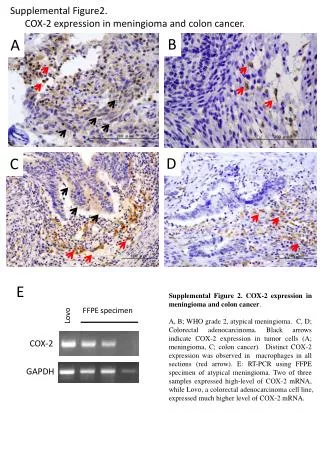
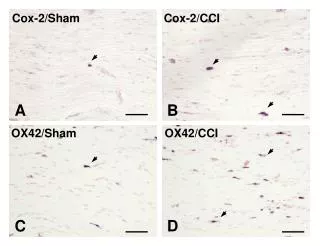
Cyclo-oxygenase II (COX-2) • Highly expressed by cells involved in inflammation(eg. macrophage, monocytes, synoviocytes) • Unregulated by bacterial lipopolysaccharides, cytokines, growth factors, tumor promoters
Cyclo-oxygenase II (COX-2) • “Inducible” form • Primarily responsible for synthesis of prostanoids involved in acute and chronic inflammatory states
COX-1 and COX-2 • However, this distinction is somewhat simplified • COX-2 also constitutively expressed under physiological conditions in severe tissues • Brain • Spinal cord • Kidney • Vascular endothelium • COX-1 also be unregulated to a certain degree in inflammation
Development of COXIBS • Theoretically, selective inhibition of COX-2 would provide • Anti-inflammatory effects • Without disrupting gastric cytoprotection and platelet function
Development of COXIBS • Hypothesis: selective inhibition of COX-2 will have • Therapeutic actions similar to NSAIDs • Without GI side effects
Thromboxane A2 (TXA2) • Synthesized by COX-1 in platelet • Vasoconstriction • Smooth muscle proliferation • Platelet aggregation
Prostacyclin (PGI2) • In contrast, PGI2, a product of arachidonic acid (AA) from COX-2 in vessel walls plays important role in homeostatic defense mechanism that promotes • Vasodilatation • Inhibition of platelet function
NSAIDS and COXIBs • NSAIDs block both COX-1 and COX-2 production to a similar extent • In contrast, COXIBs inhibits PGI2 production • Thus, COXIBs may create an imbalance between TXA2 and PGI2 • This might be the dominant mechanism that can lead to increased risk of thrombosis
Therapeutic Use • Postoperative pain • Osteoarthritis (OA) • Rheumatoid arthritis (RA) • Acute gouty arthritis • Chemoprevention • Its role in carcinogenesis, apoptosis and angiogenesis • Celecoxib approved for Rx of familial adenomatous polyp (FAP)
Gastrointestinal (GI) Tract • Common reported adverse events (AEs) were related to GI tract • Dyspepsia • Diarrhea • Nausea • Abdominal pain • Flatulence
Gastrointestinal (GI) Tract • Upper GI complications have also occurred in pts treated with COXIBs • Perforation • Ulcers • Bleedings • PUBs
Gastrointestinal (GI) Tract • Many large RCTs • COXIBs caused fewer GI AEs compared to NSAIDs • However, most, if not all, of the GI benefits will be lost in pts who take low-dose aspirin
Cardiovascular (CV) System • First evidence that COXIBs might increase CV risk emerged from VIGOR study • Rofecoxib group: 5-fold increase in thromboembolic events (primarily acute MI)
Kidney • COX-2 also constitutively expressed in kidney • Is regulated in response to alterations in intravascular volume • COXIBs may transiently • Decrease urinary Na+ excretion • Can induce mild to moderate BP elevation
Kidney • COXIBs and NSAIDs • Similar effects for kidney damage • Renal insufficiency • Na+ retention with HT • Peripheral edema • Hyperkalemia • Papillary necrosis
Dizziness Headache Flu-like symptoms Fatigue Anxiety Insomnia Other (Common) Adverse Events
Other Adverse Events • As a sulfonamide, celecoxib can cause cutaneous adverse reactions without warning even in pts with no history of sulfonamide allergy • Rash • Urticaria • Photoallergic dermatitis • Serious and potentially fetal AEs • Exfoliative dermatitis • Steven Johnson syndrome • Toxic epidermal necrolysis
Other Adverse Events • Etoricoxib 30-90 mg/day for up to 1 yr, the most frequently reported lab AEs • Increased level of SGOT • Increased level of SGPT • 1-2.1% • Hepatic dysfunction presents a contraindication • During long-term Rx with COXIBs, LFTs should be regularly monitored
Other Adverse Events • Lumiracoxib withdrawn due to severe liver damage
Conclusions • CV risks of COXIBs apparently increase with dose and duration of exposure • If COXIBs indicated • The lowest effective dose • For a limited time • BP as well as renal and hepatic function advisably monitored
Conclusions • COXIBs should not be prescribed in pts with • Ischemic heart disease • Cerebrovascular disorders (stroke) • Peripheral arterial disease