Download
1 / 27
280 likes | 629 Views
NSAIDs and COX-2-Selective Inhibitors. R3 김대언. History and Background. NSAIDs Most often used nonopiod analgesics 70 million prescriptions were given in 1991 $2.2 billion cost, worldwide over $6 billion per year First extracted from the bark of the willow tree(salix alba)

E N D
History and Background • NSAIDs • Most often used nonopiod analgesics • 70 million prescriptions were given in 1991 • $2.2 billion cost, worldwide over $6 billion per year • First extracted from the bark of the willow tree(salix alba) • Documented for use in fever since at least 1827 • Synthesized in 1899 by Felix Hoffman • In 1971, discovered aspirin acts an inhibitor of COX, preventing of PG
Contains compounds that are chemically unrelated • Grouped based on their therapeutic actions • Have analgesic, anti-inflammatory, antipyretic properties • Do not demonstrate tolerance, often more effective at controlling certain pain with fewer side effects than opioid • usually supplementating rather than replacing the role of opioid
Must be cautious • Majority of studies with patients are rheumatic or other arthritic conditions • lack of association between analgesia and anti-inflammatory effect • Dosage requirement is different • defference in the pain model used • Most studies performed in elderly patients • concomitant medical conditions • NSAIDs are actually not analgesics • antihyperalgesics
Mechanism of Action • Prostaglandin Physiology • NSAIDs provide analgesia primarily through actions outside the CNS • traditional concept • by inhibiting the formation of PG • Arachidonic acid • broken down by lipooxygenase system or COX enzyme system • PGG2 or LT pathway
Prostaglandins and Pain : Peripheral Actions • Prostaglandin • not important mediators of pain transmission • contribute to hyperalgesia peripherally by sensitizing nociceptive sensory n. endings to other mediators and by sensitizing nociceptors to respond to non-nociceptive stimuli • elevation of resting mem. potential and reduction in the firing threshold
Prostaglandins and Pain : Central Actions • direct actions at the level of the spinal cord to enhance nociception at the terminals of sensory neurons in the dorsal horn • inc. release of neurotransmitters • inc. the sensitivity of second-order neurons • inh. the release of descending inhibitory neurotransmitters
Upregulation • direct neural input • humoral factors • IL-6 trigger the IL-1b in the CNS, inc. production of COX-2 and PGE2
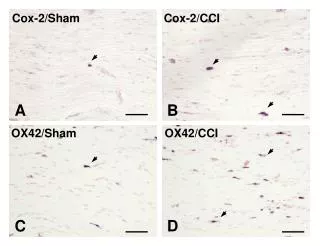
COX Isoforms • The two isoforms • about 60% identical in molecular structure • significant difference in expression and functions • Type I COX • present in variable amounts in most cells • platelet, kidney, stomach, vascular smooth m. • protecting gastric mucosa, ensuring proper platelet function, maintaining renal function • Type II COX • almost undetectable in most tissue under normal physiologic conditions • inc. during inflammation 10 to 80 folds • key in the production of hyperalgesia following injury • responsible for forming PG in the periphery and CNS • COX-3 • genetic modification of the COX-1 enzyme • play a role in CNS pain processing
NSAIDs Analgesic Actions • Preventing sensitization of peripheral nociceptors by diminishing PG formation • Inhibiting the release of inflammatory mediators from neutrophils and macrophages • Reversing the inhibition by PGs of the descending opioid-mediated noradrenergic pathways inv. in pain inhibition
COX-2 Selectivity of NSAIDs • Aspirin : irreversible inhibition of both COX-1 and COX-2 • Ibuprofen : reversible competitive inhibition of both • Flurbiprofen and indomethacin : slower, time-dependent inhibition • Celecoxib, rofecoxib, valdecoxib, etoricoxib, parecoxib : largely COX-2 selective
Enantiomer Activity • Most of the COX inhibitory activity lies with the S form • Peripheral analgesia is only mediated by the S form • R and S form both mediate central analgesia
Pharmacokinetics • Have similar pharmacokinetic characteristics • rapidly and extensively absorbed after oral administration • tissue distribution is very limited • metabolized extensively in the liver with little dependence on renal elimination • have low clearances • Toxicity may be related to their plasma half-lives • difference in efficacy is more related relative dose than property of medications
Toxicity • GI side effects added 45% to the cost of treating arthritis pts. • 72% is epigastric discomfort • Greater with inc. age • M/c reactions : GI, dermatological, neuropsychiatric • M/s reactions : GI, renal, hematologic, hepatic organ sys.
Gastrointestinal Toxicity • Gastric distress alone and actual damage with ulceration • Dyspepsia, GI bleeding, perforation, topical irritation • Alteration in GI function • mucus and bicarbonate secretion • blood flow • epithelial cell turnover and repair • mucosal immunocyte function • By topical irritation and result of inhibition of PG synthesis
Risk factors • age over 60yrs • prior history • steroid use • alcohol use • multiple NSAIDs use • first 3months of use • Sucralfate • Basic aluminium salt • Mechanisms • forming a complex with proteins at an ulcer base • stimulating PG synthesis in gastric mucosa • promoting gastric mucus secretion by PG-independent mechanism • Misoprostol • Synthetic analogue of PGE1 • H+/Na+ ATPase inhibitors • R enantiomers og NSAIDs • Nitric oxide
Renal Toxicity • 18% of pts., 6% ARF • Reduction in renal perfusion, acute interstitial nephritis, nephrotic syndrome, allergic nephritis • PGI2 and PGE2 • vasodilators • attenuate the effect of angiotensin II, renal sympathetic nerve activity, catecholamines • PGH2 and TXA2 • potent renal vasoconstrictors • Renal response to an NSAIDs : contingent on the relative amounts of these compounds
Renal prostaglandin-dependent state(RPDS) • volume depletion • low cardiac output • hepatic cirrhosis • renal ischemia • aminoglicoside toxicity • unilat. or subtotal nephrectomy • HTN and DM • Sulindac • Theoretical advantages in pt. at risk for renal toxicity • COX-2-selective inhibitors • No evidence of additional safety benefit in terms of renal toxicity
Hematologic Toxicity • TXA2 as a platelet activator and vasoconstrictor • PGI2 as a platelet inhibitor and vasodilator • Aspirin : takes 7-10days for platelet to recover • Nonaspirin NSAIDs : resolve drug is mostly eliminated • Most NSAIDs potentiate the anticoagulant activity of warfarin • by displacing the protein-bound drug • by inhibiting metabolism by hepatic microsomal enzyme • COX-2-selective inhibitors • No effects on plaetlet function even in supratherapeutic doses d/t lack of COX-2 in plaetlet
Hepatic Toxicity • 3% of pts. • Seems to be immunologic or metabolic • Sulindac and diclofenac • high risk of producing hepatic damage
Effects on Bone Healing • Both play a role in bone healing following Fx. • Reduce the rate of successful fusion • Nonselective NSAIDs have a greater effect on inhibiting bone healing than do the COX-2-selective inhibitors
Asthma • Aspirin-induced asthma(AIA) • present in 10% of asthmatics • not a true allergy • diversion of arachidonic acid breakdown from COX pathway to lipooxygenase pathway • Cox-2-selective inhibitors - not trigger this reaction
Highly Selective COX-2 Inhibitors • Celecoxib, rofecoxib, valdecoxib, etoricoxib, lumericoxib • Reduced GI morbidity and complete lack of effect on platelet function • Renal effects may be the same as nonselective NSAIDs • Rofecoxib • unique cardiovascular and renal toxicity profile : inc. in coagulability
Combination Drugs • Ibuprofen containing hydrocodone • Diclofenac with misoprostol • Ibuprofen with caffeine
Role in Acute Pain Management • Providing critical synergy to opioid analgesia • 3 areas is important : dosing, timing, toxicity • Demonstrating a ceiling effect in efficacy but remain a dose-response relationship up to ceiling • Doesn't matter whether analgesia is given before or after surgical insult • Toxicity issues relevant to the postsurgical pt. often limit their use
Future Trends • Improved understanding of the role of PG in nociception and normal physiology • Developing NSAIDs to effect isolated to the CNS with complete lack of the peripheral toxic effects • Development of nitric oxide NSAID and COX-3