Impact of 4D PET/CT Integration on Radiation Therapy Planning for Lung Cancer
This study investigates the feasibility and implications of utilizing 4D PET/CT imaging in radiation therapy planning for lung cancer patients. By analyzing two representative cases of non-small cell lung (NSCL) cancer, the research presents time-sequenced structural and functional data to support treatment planning. The study highlights the benefits of incorporating dynamic imaging protocols in evaluating tumor motion during respiration, emphasizing methods for ensuring reproducibility in breathing patterns which are crucial for accurate radiation delivery.

Impact of 4D PET/CT Integration on Radiation Therapy Planning for Lung Cancer
E N D
Presentation Transcript
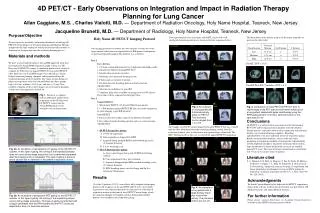
4D PET/CT - Early Observations on Integration and Impact in Radiation Therapy Planning for Lung Cancer Allan Caggiano, M.S. , Charles Vialotti, M.D. — Department of Radiation Oncology, Holy Name Hospital, Teaneck, New Jersey Jacqueline Brunetti, M.D. — Department of Radiology, Holy Name Hospital, Teaneck, New Jersey Purpose/Objective To investigate the feasibility and benefits/drawbacks of utilizing 4D PET/CT for the purpose of treatment planning in Radiation Therapy and present this time-sequenced structural/functional data visually to clinicians for incorporation into the treatment planning process. Two representative cases of patients with NSCL cancer with well-correlated respiratory patterns are shown in the time sequences below: The breakdown of the motion analysis of the tumor centroids are given in the table below: • Holy Name 4D PET/CT Imaging Protocol • Our imaging protocol was broken into two separate sessions due to the large amount of data that was required for our IRB protocol comparison of gated and ungated imaging. The protocol was as follows: • Day 1 • Part 1 RT Sim • 1. Creation of immobilization device (wingboard with Alpha-cradle a requirement). Must fit through PET bore! • 2. Identification of patient isocenter. • 3. Breathing assessment and training session • 4. Fluoroscopy assessment of motion. • 5. Establish baseline breathing pattern and intra-fraction reproducibility. • 6. Selection of candidates for gated RT. • 7. Simulator films taken at middle of gating interval (50% phase). These films will be compared to daily port films. • Day 2 • Ungated PET/CT • 1. Whole body PET/CT (15-20 mCi FDG/60 min uptake). • 2. 1-2 bed position ungated PET/CT RT Sim (for study comparison to gated imaging as per IRB protocol). • Gated PET/CT • 3. Passive reflective marker is placed on abdomen of patient. • 4. Re-validate baseline breathing pattern and assess inter-fraction reproducibility. • 5. 4D PET (Prospective gating) • A. 1 FOV 2D acquisition • B. Data acquisition is triggered by RPM • C. Acquired during multiple RPM coached-breathing cycles (5-8 minute duration) • D. 6.5 sec breathing cycle • 6. 4D CT (Retrospective gating) • A. Area scanned larger than gated 4D PET for full lung volumes. • B. Cine acquisition/4 slices per revolution • C. Acquired during multiple RPM coached-breathing cycles (4-5 minute duration) • D. RPM breathing traces saved to floppy and ftp’d to Advantage Workstation. Materials and methods We have accrued eighteen patients into an IRB-approved study that investigates the Varian RPM respiratory gating system on a GE Discovery LS PET/CT scanner. A simulation protocol was created to compare the differences in ungated PET/CT versus gated PET/CT (4D). Both sets of CT and PET images were utilized on a Varian Eclipse treatment planning computer and incorporated into the treatment planning for these patients. The tumor motion during all phases of respiration were assessed and broken into three groups: high (>2.0 cm), medium (1.0-2.0 cm), and low (<1.0 cm). New methods of display of these gated images on our treatment planning system were investigated for clinical use. Pre-RT, SUV = 16.0 Post-RT Post-RT (7 months), SUV = 4.1 Fig. 1. Picture of a volunteer with an abdominal marker block in position on the GE Discovery LS PET/CT scanner and the Varian RPM gating system attached to the treatment table. Fig. 3. An example of a lung patient with 4 discrete activity areas on PET/CT. The maximum motion ranged from 1 to 2 cm. Fig. 5. Comparison of initial PET from PET/CT prior to radiotherapy to the PET scan at the 6-month follow-up for a lung patient treated with gated radiotherapy using the RPM gating system. The tumor centroid motion for this case was 3.0 cm. Conclusions 4D PET/CT is a useful clinical assessment tool for determining BTV/GTV and/or organ motion in properly selected radiation therapy patients, especially when used in conjunction with dynamic displays on treatment planning computers. Breathing reproducibility is the most important factor for respiratory gating. Breath synchronization methods, such as audio and video prompting, are important methods of ensuring this reproducibility of both amplitude and phase. In patients with large tumor motion, large uncertainties in tumor localization can occur on standard ungated CT scans. The range of tumor centroid motion varied from 0 to 3.0 cm in our current series of patients. An example of a NSCLC patient imaged with gated PET/CT that was overlaid with the dose distribution from the treatment planning system. Note the excursion of tumor close to the inferior and superior edges of the field. The MLC blocking used for this case was based the ungated PET/CT acquisition. Fig. 2a. An illustration of retrospective CT gating on the GE PET/CT scanner. In this type of gating, the sorting of the respiratory phases does not occur during image acquisition, but is performed separately after the imaging study is completed. This type of gating is prone to errors caused due to variations in the patient’s respiratory motion. Literature cited S. A. Nehmeh, Y. E. Erdi, G. Mageras, T. Pan, E. Yorke, H. Mostavi, D. Hurley, O. Squire, J. L. Ham, H. Schroeder, S. M. Larson, K. E. Rosenzweig, “Improved accuracy in image co-registration and tumor quantitation of pulmonary lesions of NSCL patients by respiratory correlated acquisition on PET/CT,” J. Nucl. Med. 44, No. 124 (2003). Results 15 of the 18 patients (83.3%) were able to fully complete the imaging protocol. All ten phases of the gated PET and CT were successfully registered to each other and presented to clinicians for evaluation of respiratory motion in the form of fused PET/CT movie loops, which the clinicians thought were highly useful in determining whether patients were candidates for respiratory gating. Acknowledgments We thank Cynthia Mento for her help with the PET/CT acquisitions. Some of the software used for this presentation was provided by GE Medical Systems, and Varian Medical Systems. Fig. 4. An example of a lung patient with a large primary lesion plus nodal chain activity. The maximum motion was 3.0 cm. For further information Please contact caggiano@holyname.org. An online version of poster is available at the ASTRO electronic poster website. Fig. 2b. An illustration of prospective PET gating on the GE PET/CT scanner. In this type of gating, the sorting of the respiratory phases occurs during image acquisition. This type of gating is performed with a trigger generated from the RPM system and the PET counts are deposited in bins of a fixed time duration.