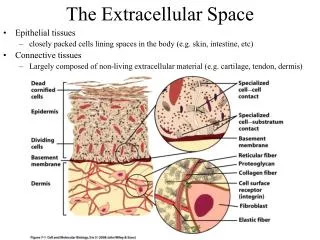
Extracellular Pathology
Extracellular Pathology. Amyloidosis Pathological calcification Ageing. Amyloid and Amyloidosis. A Set of Disorders: The main feature is the extracellular deposition of proteins arranged in the form of a Beta-pleated sheet “Amylum” Latin for starch Term first used By Virchow in 1854

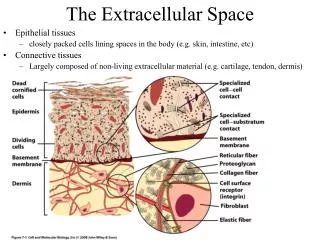
Extracellular Pathology
E N D
Presentation Transcript
Extracellular Pathology Amyloidosis Pathological calcification Ageing
Amyloid and Amyloidosis • A Set of Disorders: The main feature is the extracellular deposition of proteins arranged in the form of a Beta-pleated sheet • “Amylum” Latin for starch • Term first used By Virchow in 1854 • Protein….Friedreich and Kekule. 5 years later
Amyloidosis • Amyloidosis is a clinical disorder caused by extracellular deposition of insoluble abnormal fibrils that injure tissue. • The fibrils are formed by the aggregation of misfolded, normally soluble proteins. • In humans, about 23 different unrelated proteins are known to form amyloid fibrils.
Amyloidosis • All types of amyloid consist of a major fibrillar protein that defines the type of amyloid (approximately 90%) plus various minor components. • Although each type of fibril may be associated with a distinct clinical picture, all share certain physical and pathologic properties
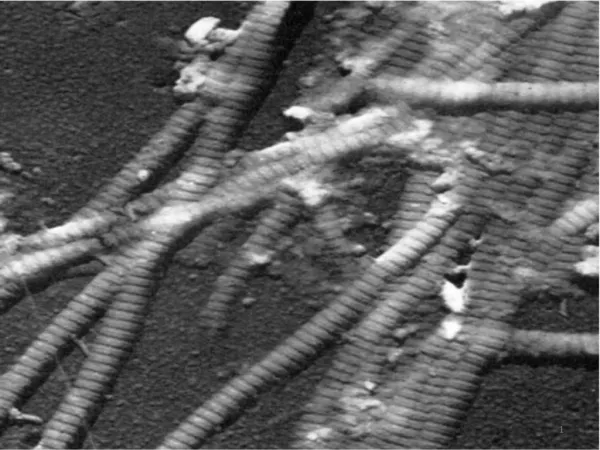
Organs affected by amyloid: Larger, Paler, Firmer • How do we identify Amyloid in tissues? Macroscopically (Grossly) Waxy, Sharper cut edges, Lugol’s iodine (black). Microscopically: Light Microscopy- Amyloid is eosinophilic and stains with Congo Red Polarized light: Apple Green Birefringence. Electron Microscopy: Rigid non branching fibrils (7.5 nm to 10 nm in diameter)
The Beta- Pleated sheet is the unifying feature of the amyloidoses Basis of 1) Congo Red reaction 2) Fibrillar ultrastructure 3) Resistance to proteolytic digestion
Why? • Protein Misfolding • Intrinsic tendency to misfold (Transthyretin) • Misfolding and aggregation at high concentration (Beta Microglobulin) • Point mutations (Hereditary amyloidosis) • Review: Molecular mechanisms of amyloidosis. Merlini G, Bellotti V. NEJM August 2003 349:583-96
Classification • Older classifications: 1° and 2° • More useful to classify on the basis of: 1) Nature of protein involved 2) Anatomical distribution 3) Inherited or acquired
Acquired Systemic Amyloidosis 1) Amyloidosis of immune origin. AL type • Acquired, Systemic form • Protein precursor is usually immunoglobulin light chain. • Occurs in association with a monoclonal (i.e. neoplastic) proliferation of B lymphocytesor plasma cells e.g. • Myeloma (Lambda chains) • Waldenstrom’s macroglobulinaemia (LPL)
AL amyloid proteins : Intact immunoglobulin light chain or the amino terminal fragment of a chain or both. (mostly lambda chains) 90% of these patients have Bence Jones proteins Amyloid accumulation: Two step process 1) Secretion of excess amounts of monoclonal light chain 2) Conversion to Beta pleated form.
Clinical features • Middle to old age • M>F • 90% have a Bence Jones protein • Bone marrow = excess plasma cells • Manifestations Neuropathy, Restrictive Cardiomyopathy, Skin manifestations, Polyarthropathy,Macroglossia, Carpal Tunnel Syndrome • (Heart, CNS, Joints, Skin, Tongue, Soft Tissues)
Immunofluorescence microscopy with antibody to the lambda light chain.
Cardiac 2nd Year Pathology 2009
2) Haemodialysis associated Amyloid Acquired, systemic Protein is Beta-2-microglobulin. Normally broken down by kidneys A naturally occurring “amyloidogenic” protein not filtered by dialysis membranes After 7 years on dialysis 30% of patients get Carpal Tunnel Syndrome (after 10 years 50%) Joints, synovium, tendon sheaths Acquired Systemic Amyloidosis
Acquired Systemic Amyloidosis 3) Reactive Systemic Amyloidosis • Also known as secondary amyloid or AA type amyloid • Acquired, systemic form • Protein precursor is serum amyloid A (SAA) • Acute phase reactant which markedly increases with tissue injury or inflammation under the influence of IL1, TNF and IL-6 • AA is a cleavage product of SAA. • Distribution of amyloid: kidney, liver, spleen, adrenals, thyroid + many other tissues. • Diagnosis: Rectal Biopsy
1) Chronic infection: T.B., Leprosy, Syphilis, Chronic osteomyelitis, Bronchiectasis 2) Chronic inflammation Reiter’s disease, Whipple’s disease 3) Chronic autoimmune disease: R.A., I.B.D., Connective Tissue Disease 4) Long standing paraplegia. (UTI) 5) Neoplasms: Renal adenocarcinoma and Hodgkin’s disease Disease Associations:
Hereditary Systemic Amyloidosis • Rare. • Most common: Familial Mediterranean Fever. • Less common: Three types: • Neuropathic. • Cardiopathic. 3) Nephropathic. The Amyloid protein is usually Transthyretin (Prealbumin). Transthyretin is also associated with a form of Amyloid known as Systemic Senile Amyloid, where amyloid is systemically deposited, mainly in the heart in elderly individuals.
Familial Mediterranean Fever • Commonest form of hereditary systemic amyloidosis • Autosomal Recessive, Gene on Chromosome 16 • AA type amyloid • Two manifestations of the disease: • Short febrile attackswith pain mimicking pleurisy, peritonitis or synovitis • Amyloidosis: Manifest early in life • Death before 40 without Renal Transplant • Treated with Colchicine (Stabilization of inflammatory cells)
Localized amyloidosis • Endocrine associated: Pituitary - age related Islets of Langerhans - NIDDM related Medullary Carcinoma of Thyroid (Calcitonin) • Intacerebral: Alzheimer’s, Spongiform Encephalopathy
Amyloid angiopathy 2nd Year Pathology 2009
Pathological Calcification Dystrophic Calcification Metastatic Calcification Idiopathic Calcification
Dystrophic Calcification • Normal serum calcium/phosphate • Nonviable or dying tissues • Occurs in atherosclerosis, damaged valves, necrosis (coagulative, caseous, liquefactive), Leiomyomas • Monckeberg’s medial sclerosis • Intracellular / Extracellular • Two phases: Initiation and Propagation
Dystrophic Calcification Tricuspid valve Stomach
Metastatic Calcification • Must be associated with elevated Calcium. • Occurs in vital tissues • Aetiology: • Increased PTH • Hyperparathyroidism • Bone destruction • Tumour (MM, Leukaemia), Skeletal Mets (Breast Ca.) • Increased bone turnover (Pagets), Immobilisation. • Vitamin D related disorders • Excess Vitamin D • Sarcoidosis • Renal Failure • Retention of Phosphate, (secondary HyperPTH)
Metastatic Calcification • Kidney: Around tubules - Renal Failure. • Lung: Alveolar walls. • Stomach: Fundal glands. Identification of Calcium: Von Kossa 2nd Year Pathology 2009
Hyperparathyroidism • Primary, Secondary, Tertiary • 1° = Increased bone re-absorbtion and mobilization of calcium from bone Increased renal tubule re-absorption. Increased Vit. D activity “ Bones, stones , (psychic moans) and abdominal groans” 2nd Year Pathology 2009
Aetiology: 1) Parathyroid adenoma. 75% 2) Hyperplasia. 10-15% 3) Parathyroid carcinoma <5% (MEN 1 or MEN2a) Secondary: Renal Failure, Osteomalacia.
Ageing • Aging is NOT a disease • The changes that occur with aging make aged persons more susceptible to disease • Aging is probably multifactorial involving both internal (Genetically programmed) and external (Tissue damage) factors that combine to exert their effects
Theories of Aging • Cellular Changes. • There is cumulative free radical damage to DNA and to proteins (perhaps due to lack of antioxidants). • Genetics • Another theory suggests that aging is determined by genetic programming and malfunction. • 1962 The Hayflick phenomenon. Telomeres and Telomerase • Progeria (Werner’s syndrome). DNA Helicase • Loss of Homeostasis • Environmental Stress • Neuroendocrine Dysfunction • Nutrition
Organ Systems • Central Nervous System • Stroke. • Alzheimer’s. • Neuronal loss. • Eye • Cataracts. • Presbyopia. • Ear • Presbycusis. 2nd Year Pathology 2009
Cardiovascular System • Atheroma • Calcification (Senile calcific aortic sclerosis) • Senile Amyloid. • Urinary Tract • Decreased GFR. • Increased UTI in women. • Musculoskeletal System • Decreased bone mass. • Osteoarthritis.
Genital Tract • Menopause leads to atrophy of ovaries, uterus, and breasts. The epithelium of the vagina and vulva also become thinner. • Prostatic Hyperplasia. • Skin • Decreased elasticity. • Senile lentigines 2nd Year Pathology 2009
Timing of Aging: Telomeres • Telomerase stabilizes telomere lengths • Active in germ cells, absent in most somatic cells • May be reactivated in cancer cells • When cells replicate, small portion of telomere not duplicated • Telomere shortening – growth checkpoint = signal for cell to become senescent • Mechanism for cells to count their divisions