Download

1 / 38
380 likes | 400 Views
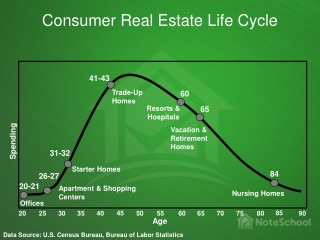
Ministry of Finance's report on healthcare spending in Slovakia over the past decade, highlighting inefficiencies and areas for improvement in hospitals, medicine spending, and health insurance.

E N D
Spending ReviewHealthcare State of play May 30th 2016
Summary – Healthcare According to Ministry of Finance Over the past 10 years, spending on healthcare in Slovakia has grown significantly, however, healthcare results are poor compared to Hungary, Poland, Czech Republic (amenable mortality, life expectancy) Funds available in healthcare are perceived as sufficient We spend a lot on medicines Hospitals are inefficient (excess capacities and overprices purchases) Inefficiency in healthinsurancemarket We spend more than other countries on diagnostic imaging, laboratories, transportation and medical rescue services Data largely unavailable – responsible bodies reluctant to share data
Terms of Reference • Goal in terms of healthcare results: • Lowering amenable mortality to the average level of Hungary, Poland and the Czech Republic by 2020 (1872 less amenable deaths annually) • Fiscal goals: • Spending growth at inflation level • Increase of capital spending of hospitals by 633 mln. EUR over four years (to cover the construction of 3 new hospitals and the renovation of 5 large hospitals)
Total spending Total healthcare spending (% GDP) Total healthcare spending (per capita, PPPs, USD, current prices)
Avoidable mortality • High amenable mortality • Deaths that can be prevented by healthcare interventions • Compared with V3, there are 1890 more deaths annually in Slovakia Amenable mortality (standardized death rate per 100 000 inhabitants)
Life expectancy Low life expectancy (women at birth) Difference in life expectancy (women compared with men at birth)
Capital spending Investment spending in healthcare (per capita, PPPs, USD, current prices) Investment spending as a share of total spending (%)
Breakdown of spending in 2013 • We spend too much on medical goods • We spend too much on ancillary services • We spend more on ambulatory care than the V3 countries • We spend less on inpatient care
We’re looking for savings in four major areas • Hospitals • Medicinesand othermedicalgoods • Health insurance companies • Diagnostic imaging, laboratories, transportation and medical rescue services
Hospital beds Number of beds (per 1000 inhabitants) Bed occupancy (% of available beds)
Hospitals • Are hospitals run efficiently? • Benchmarking of hospitals´ operationalexpenditure (lookingforinternationalbenchmarks) • Data envelopment analysis of inputs and outputs/ results (usefulexercise?), recommendations for greater efficiency • How much could hospitals save if they purchased services at prices achieved by most efficient hospitals/ market prices? • Benchmarking of unit prices of services (data publicly available) and quantification of achievable savings
Consumption of medical goods and pharmaceuticals Consumption of pharmaceuticals and other medical non-durables ( per capita, PPPs, USD, current prices) Consumption of medical goods, including pharmaceuticals (per capita, PPPs, USD, current prices)
Medicines and othermedicalgoods I • Does health insurance cover drugs that do not fulfill coverage conditions in terms of cost efficiency? • Analysis of cost efficiency of expensive drugs, quantification of savings achievable by fulfilling cost efficiency conditions • Review whether pharmacoeconomic analyses of drugs approved for reimbursement after 2011 meet the statutory requirements • What savings could be achieved if special medical materials (implants, etc.) in each category were only fully reimbursed up to a particular level and co-payments were introduced for more costly alternatives? • Quantification of savings with reimbursement at level of cheapest and median good in each category
Medicines and othermedicalgoods II • Can medicine consumption and spending be cut by introducing prescription guidelines? • Analysis of differences in medicine prescription for similar diagnoses • Is our medicine consumption too high? • International comparison of consumption of medicines and medical goods (inpatients drugs, outpatient drugs, etc.) in specific categories • Comparison of declared morbidity and drug consumption
Healthinsurancemarket Spending on health administration and health insurance (per capita, PPPs, USD, currentprices)
Health insurance companies • Does the distribution of health insurance contributions among health insurance companies reflect their costs? • Analysis of redistribution mechanism • Are health insurance companies managed in an efficient manner? • Comparison of operating costs and quantification of achievable savings (lookingforinternationalbenchmarks) • Does the health insurance market allow the creation of economic rent? • Analysis of health insurance companies profits (lookingforinternationalbenchmarks)
Spending on ancillary services Spending on laboratories and diagnostic imaging (per capita, PPPs, USD, current prices) Spending on transportation and medical rescue services* (per capita, PPPs, USD, current prices) *The comparatively high spending on transportation and medical rescue services in Slovakia can be explained by high private spending, which amounts to almost half of total spending. In other countries these services are mostly covered by public spending.
Diagnostic imaging, laboratories, transportation and medical rescue services • Are we paying more than other countries? • Benchmarking of unit prices in Slovakia and neighboring countries (lookingforinternationalbenchmarks) • Quantification of achievable savings with prices at level of surrounding countries
Inputs Workforce & salaries • Too few nurses, number declining further; underpaid • Stable number of physicians, close to EU average in number and pay • Too many specialists • Too few GPs
Outputs Consultations & hospital discharges • Too many consultations per inhabitant • Number of hospital discharges per inhabitant slightly higher than EU average • Average length of hospital stay below EU average Prevention • Breast cancer and cervical cancer screening below average
Work force • Too few nurses • Stable number of physicians, dentists and pharmacists
Nurses • The number of nurses has been falling since 2007 • The discrepancy between the number of nurses in Slovakia and in other countries has been growing since 2004
Physicians and physicians’ age Number of professionally active physicians excluding dentists (per 1000 inhabitants)
General practitioners and specialists General practitioners and specialists in 2007 (per 1000 inhabitants) • Slovakia has too few general practitioners • Number of specialists is higher than average • Number of surgeons, obstetricians and gynecologists is higher than in other countries
Physicians and nurses’ wages Income of general practitioner – employed (% of average wage) Income of nurse employed in hospital (% of average wage)
Medical Technology Medical Technology (2013, per million inhabitants) Medical technologies in hospitals (H) and ambulatory care (A) (2013, %)
Ambulatory healthcare Number of consultations (per inhabitant) • Number of consultations is continuously higher than average (with the exception of 2005)
Inpatient care Number of hospital discharges (per100 000inhabitants) Average length of hospital stay (number of days)
Surgical procedures Less surgical procedures compared to benchmarks (2013, per 100 000 inhabitants)
Prevention – cancer Breast cancer screening ( % of population aged 50-69) Cervical cancer screening ( % of population aged 50-69)