Download
1 / 9
110 likes | 550 Views
Successful management of keratomycosis in a case of uncontrolled Ocular C icatricial Pemphigoid. Hatem Kobtan MD FRCS (Ed) ( Glasg ) Dina kobtan MD MSC Cairo University. The authors have no financial interest to disclose. ASCRS San Francisco 2009 . Purpose .

E N D
Successful management of keratomycosis in a case of uncontrolled Ocular CicatricialPemphigoid Hatem Kobtan MD FRCS (Ed) (Glasg) Dina kobtan MD MSC Cairo University The authors have no financial interest to disclose ASCRS San Francisco 2009
Purpose • To report the management of refractory keratitis in a case of undiagnosed advanced ocular cicatricialpemphigoid (OCP).
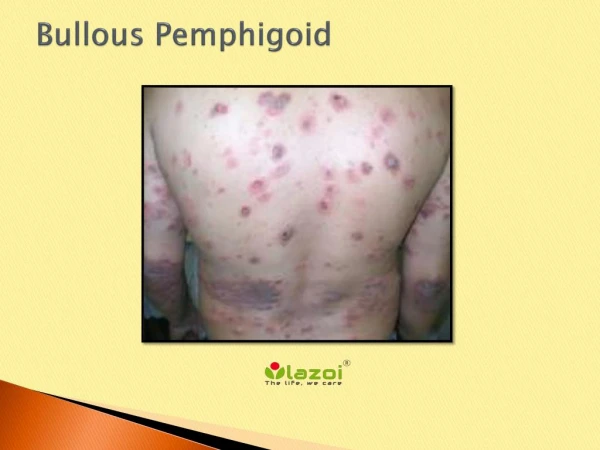
Material and Methods • 60 year old farmer presents with pain and diminution of vision of two months duration in his right eye . • Examination revealed Rt central corneal infiltration with feathery margins, extensive stromal vascularization and descmetocele formation. • A chronic cicatrizing conjunctivitis with fornix shortening, symblepheron, ankyloblepheron and multiple rubbing lashes was noted in both eyes. • Visual acuity of light perception in the Rt eye ,6/60 in Lt eye.
Corneal scraping with culture and sensitivity was performed on the Rt eye. • Conjunctival biopsy with immunohistochemistry was performed on the Lt eye. • Topical Amphotericin B and systemic Itraconazole were initiated on clinical suspicion of fungal keratitis. • Systemic immunosuppressives were instituted after the resolution of keratitisand the diagnosis of OCP by immunohistochemistry.
Results • Culture plates grew Aspergillus. The patient’s keratomycosis resolved with topical and systemic antifungal therapy. • Vision improved from hand motion to ambulatory vision after resolution of the keratitis. • Clinical suspicion of OCP was confirmed with immunohistochemistry of conjunctival biopsy from the other eye which showed IgG at the epithelial basement membrane zone and low dose systemic steroids combined with azathioprine were started.
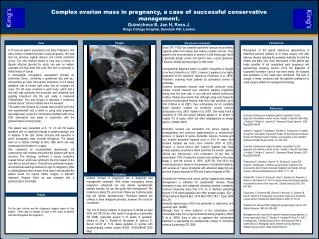
5-2-2005 5-2-2005 24-7-2005 Rt central corneal infiltration with feathery margins, extensive vascularization and descmetocele formation. Chronic cicatrizing conjunctivitis with fornix shortening, symblepheron, ankyloblepheron and multiple rubbing lashes. Five months later following resolution of the keratitis with formation of a paracentralleucoma and the initiation of Imunosuppressive therapy (low dose steroid combined with azathioprine) to control of the OCP activity. 27-3-2005
31-7-2005 11-6-2006 Lt eye showing thickening of the lid margin with loss of lashes, ankyloblepheron, conjunctival hyperemia, fornix shortening and corneal neovascularization Lt eye 10 months later showing the resolution of the lid and conjunctival inflammation following systemic immunosuppressives(low dose steroid and azathioprine)
Conclusion • The compromised ocular surface in patients with uncontrolled OCP places them at an increased risk of microbial keratitis. • Proper diagnosis and selection of the appropriate anti-microbial can be sight saving in cases of refractory keratitis associated with advanced OCP. • Systemic immuosuppression is mandatory once the infection is controlled to limit the progression of the ocular surface disease. • Our reported case is unique due to the difficulty in laboratory confirmation of clinically suspected keratomycosis and the relatively rare occurrence of OCP.
References • Barbara Iaccheri, Manolette Roque, Tito Fiore, Thekla Papadaki, Benjamin Mathew, StefanosBaltatzis, Barry Emara, A. C. Tokarewicz, and C. Stephen Foster. Ocular Cicatricial Pemphigoid, Keratomycosis, and Intravenous Immunoglobulin Therapy. Cornea 2004;23: 819– 822. • Karla J. Johns, Denis M. O’Day. Pharmacologic management of keratomycoses Survey of ophthalmology 1988; 33: 178- 188. • Valerie P.J. Saw, John K.G. Dart, SaaehaRauz, Andrew Ramsay, CateyBunce, Wen Xing, Patricia G. Maddison, Melanie Phillips. Immunosuppressive Therapy for Ocular Mucous Membrane Pemphigoid: Strategies and OutcomesOphthalmology 2008; 115: 253-261.