Download
1 / 1
10 likes | 212 Views
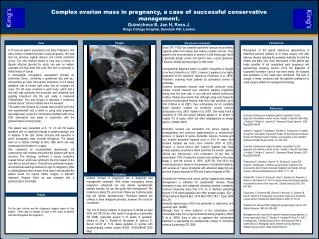
Complex ovarian mass in pregnancy, a case of successful conservative management. Guimicheva B, Jan H, Ross J. Kings College Hospital, Denmark Hill, London. Images. Case. Conclusions. Discussion continued.

E N D
Complex ovarian mass in pregnancy, a case of successful conservative management. Guimicheva B, Jan H, Ross J.Kings College Hospital, Denmark Hill, London Images Case Conclusions Discussion continued.. A 37-year-old patient presented to our Early Pregnancy Unit with a history of abdominal pain in early pregnancy. She had had one previous vaginal delivery and normal menstrual cycles. The only medical history of note was a history of Bipolar affective disorder for which she was on sodium valproate and high dose folic acid. She had no personal or family history of cancer. A transvaginal sonographic assessment showed an anteverted uterus, containing a gestational and yolk sac, representing an early intra-uterine pregnancy of 4-5 weeks gestation, with a normal right ovary and an enlarged left ovary. The left ovary contained a cystic lesion, which had a thin wall, was unilocular and avascular, and contained solid papillary projections into the cyst cavity. It measured 70x62x54mm. This was thought to represent a borderline ovarian tumour. Tumour markers were not elevated. The patient was followed up 2 weeks later at which point she was asymptomatic and a viable on going early pregnancy was diagnosed. A plan for conservative treatment with close USS observation was made in conjunction with the gynaecological oncology team. The patient was rescanned at 8, 13, 24 and 36 weeks gestation with no significant change in symptomatology, size or features of the cyst. Senior clinicians with expertise in pelvic sonography were involved throughout. The patient went on to deliver normally at term, after which she was reassessed and booked for surgery. She underwent an uncomplicated laparoscopic left oophrectomy with omental and peritoneal biopsies with good recovery. The histology confirmed a serous borderline ovarian tumour, which was confined to the inner aspect of the cyst with no microinvasion. Omental and peritoneal biopsies, and peritoneal washings showed no sign of malignancy. After a multidisciplinary team review of the case it was decided the patient would not require further surgery or adjuvant treatment. Regular follow up was arranged with a gynaecological oncologist. Recognition of the typical ultrasound appearances of borderline tumours allowed us to delay surgery until after delivery, thereby reducing the potential morbidity for both the mother and baby. Very close observation of this patient was made possible of our specialised early pregnancy and gynaecology scanning service. Once the diagnosis of suspected borderline tumour had been made, the features and symptoms of the mass were monitored. The lack of change in these, combined with the patient's preferance to avoid surgery settled our management strategy. Since 1971 FIGO has classified borderline tumours as an entirely separate entity from benign and invasive ovarian tumours. They appear to be more prevalent in women of child baring age, follow a generally benign course and tend to have a good prognosis. Therefore, fertility sparing surgery is often used. Sonographical diagnosis based on pattern recognition is thought to be best (Valentin et al, 2001), however it appears to be highly dependent on the operators' experience (Timerman et al, 1994). Therefore, scanning these patients by specialised centres is preferable. Common sonographic features used include unilocular cysts, positive ovarian crescent sign, extensive papillary projections arising from the inner wall, or cyst with well defined multilocular nodules. Studies have shown that, although using such frequently occurring morphological features may have high specificity, up to 0.94 (Yazbek et all 2007), they unfortunately do not constitute highly sensitive markers for borderline ovarian tumours (Exacoustos et al, 2005/ Yazbek et al, 2007). One study found a sensitivity of 0.69 and typical features appear to be absent in roughly 1/3 of cases, which are often misdiagnosed as benign lesions. (Yazbek 2007) Borderline tumours are subdivided into serous (typical or micropapillary) and mucinous (gastrointestinal or endocervical) tumours. In respect to serous borderline tumours, invasive and non invasive peritoneal implants occur in 35% of cases. Non invasive implants are much more common (78% vs 22%), however, a serous tumour with invasive implants may have profuse papillary projections which perforate the ovarian capsule without any macroscopic solid component. At the time of presentation, 70% of borderline tumours are confined to the ovary (stage I), and the survival is 100%. (AJR:194, Feb 2010) the overall prognosis is based on the presence of peritoneal implants, with survival at 7 years of patients with advanced stage tumours and non invasive implants of 95% and invasive implants of 66%. Generally the evidence and current opinion suggests that surgical management is indicated for symptomatic masses, those increasing in size and complexity indicating possible complexity. Tumours measuring more that 5-10 cm in diameter persisting beyond 15/16 weeks gestation also often prompts surgery. (Eur J Obstet Gynecol Reprod Biol. 2010 Mar;149(1):18-21. Epub 2009 Dec 29) Generally laparoscopy is felt to be preferable to laparotomy, and generally safe. (SAGE) Although there is some evidence of low complication and miscarriage rates from surgical treatment during pregnancy (Balci O et al, 2008), there is also an argument that conservative treatment is appropriate for asymptomatic benign or borderline tumours.(Leiserowitz GS, 2006 References Accuracy of ultrasound subjective 'pattern recognition' for the diagnosis of borderline ovarian tumors. Yazbek J, Raju KS, Ben-Nagi J, Holland T, Hillaby K, Jurkovic D. Ultrasound Obstet Gynecol. 2007 May;29(5):489-95 Valentin L, Hagen B, Tingulstad S, Eik-Nes S. Comparison of ‘pattern recognition’ and logistic regression models for discrimination between benign and malignant pelvic masses: a prospective cross validation. Ultrasound Obstet Gynecol 2001; 18: 357–365. Accuracy of ultrasound subjective 'pattern recognition' for the diagnosis of borderline ovarian tumors. Yazbek J, Raju KS, Ben-Nagi J, Holland T, Hillaby K, Jurkovic D. Ultrasound Obstet Gynecol. 2007 May;29(5):489-95 Timmerman D, Verrelst H, Bourne TH, De Moor B, Collins WP, Vergote I, Vandewalle J. Artificial neural network models for the preoperative discrimination between malignant and benign adnexal masses. Ultrasound Obstet Gynecol 1999; 13: 17–25. Gotlieb WH, Soriano D, Achiron R, Zalel Y, Davidson B, Kopolovic J, Novikov I, Ben-Baruch G. CA 125 measurement and ultrasonography in borderline tumors of the ovary. Am J Obstet Gynecol 2000; 183: 541–546. Exacoustos C, Romanini ME, Rinaldo D, Amoroso C, Szabolcs B, Zupi E, Arduini D. Preoperative sonographic features of borderline ovarian tumors. Ultrasound Obstet Gynecol 2005; 25: 50–59. Shepherd JH. Revised FIGO staging for gynaecological cancer. Br J Obstet Gynaecol 1989; 96: 889–892 Management and outcomes of adnexal masses during pregnancy: a 6-year experience. Balci O, Gezginc K, Karatayli R, Acar A, Celik C, Colakoglu MC. J Obstet Gynaecol Res. 2008 Aug;34(4):524-8. Leiserowitz GS, Managing ovarian masses during pregnancy. Obstetric Gynecol Surv. 2006 Jul;61(7):463-70. Discussion Ovarian tumours in pregnancy are a diagnostic and management challenge. With routine sonography during pregnancy, ultrasound not only detects asymptomatic adnexal masses, but can also guide their management. The incidence is about 2%, and most of these are functional cysts that will resolve spontaneously. Persistent masses are unlikely to have malignant potential, however, this must be considered. The role of tumour markers in pregnancy is limited as beta HCG and CA125 are often raised in pregnancy (Leiserowitz GS 2006), especially around 11-14 weeks of gestation. (Aslam N, Ong C, Woelfer B, Nicolaides K, Jurkovic D. Serum ca125 at 11-14 weeks gestation in women with morphologically normal ovaries. BJOG. 107(5):689-90 2000 May) Images On the next column are the ultrasound images taken for this patient. There was no change on each of the scans at several intervals throughout the pregnancy.