U.T.I Cystitis & Pyelonephritis
370 likes | 1.03k Views
U.T.I Cystitis & Pyelonephritis. Dr. Abdelaty Shawky Dr. Gehan Mohamed. * Predisposing factors: . B ladder calculi. U rinary obstruction. D iabetes mellitus. Instrumentation. immune deficiency.

U.T.I Cystitis & Pyelonephritis
E N D
Presentation Transcript
U.T.ICystitis & Pyelonephritis Dr. Abdelaty Shawky Dr. Gehan Mohamed
* Predisposing factors: • Bladder calculi. • Urinary obstruction. • Diabetes mellitus. • Instrumentation. • immune deficiency. • Patients receiving cytotoxic antitumor drugs, such as cyclophosphamide, sometimes develop hemorrhagic cystitis
* Causative organisms: • The common etiologic agents of cystitis are: Escherichia coli, Proteus, Klebsiella, and Enterobacter. • Women are more likely to develop cystitis as a result of their shorter urethra. • Tuberculouscystitis is almost always a sequel to renal tuberculosis.
Candida albicans (Monilia) and, much less often, cryptococcal agents cause cystitis, particularly in immunosuppressed patients or those receiving long-term antibiotics. • Schistosomiasis (Schistosomahaematobium) is common in certain Middle Eastern countries, notably Egypt. • Viruses (e.g., adenovirus), Chlamydia, and Mycoplasma may also be causes of cystitis.
* Clinical presentation of cystitis: - All forms of cystitis are characterized by a triad of symptoms: 1. Frequency, which in acute cases may necessitate urination every 15 to 20 minutes. 2. Lower abdominal pain localized over the bladder region or in the suprapubicregion. 3. Dysuria—pain or burning on urination.
Associated with these localized changes, there may be systemic signs of inflammation such as elevation of temperature, chills, and general malaise.
Cystitis may be precede pyelonephritis. • Cystitis is sometimes a secondary complication of some underlying disorder such as prostatic enlargement, cystocele of the bladder, calculi, or tumors. These primary diseases must be corrected before the cystitis can be relieved.
* Types of cystitis: 1. Hemorrhagic cystitis: When there is a hemorrhagic component, This form of cystitis sometimes follows radiation injury or antitumor chemotherapy and is often accompanied by epithelial atypia. Adenovirus infection also causes a hemorrhagic cystitis.
2. Suppurative cystitis: accumulation of large amounts of suppurative exudate . 3. Ulcerative cystitis: there is ulceration of large areas of the mucosa, or sometimes the entire bladder mucosa.
4. Chronic cystitis: due to persistent infection. The mucosa appears red, friable, granular, sometimes with ulcerated surface. Chronicity of the infection gives rise to fibrous thickening in the muscularispropria and consequent thickening and inelasticity of the bladder wall. 5. Follicular cystitis: Characterized by the aggregation of lymphocytes into lymphoid follicles within the bladder mucosa and underlying wall.
6. Eosinophilic cystitis: manifested by infiltration of the submucosa by eosinophils together with fibrosis and occasionally giant cells. Most cases of eosinophilic cystitis represent nonspecific subacute inflammation, although, rarely, these lesions are manifestations of a systemic allergic disorder.
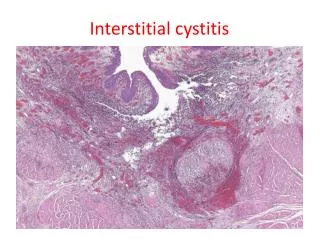
7. Interstitial Cystitis (Hunner Ulcer): • This is a persistent, painful form of chronic cystitis occurring most frequently in women and associated with inflammation and fibrosis of all layers of the bladder wall. • The condition is of unknown etiology but is thought to be of autoimmune origin, particularly because it is sometimes associated autoimmune disorders.
It is characterized clinically by intermittent, often severe, suprapubic pain, urinary frequency, urgency, hematuria, and dysuria without evidence of bacterial infection. Some but not all patients exhibit morphologic features of chronic mucosal ulcers (Hunner ulcers).
* Microscopically: Inflammatory cells and granulation tissue involve the mucosa, lamina propria, and muscularis mucosa, with prominent mast cells.
Interstitial cystitis Giant cell
8. Polypoid Cystitis: • Polypoid cystitis is an inflammatory condition resulting from irritation to the bladder mucosa usually by indwelling catheters. The urothelium is thrown into broad polypoid projections as a result of marked submucosal edema.
*Def:inflammation of the renal pelvis and renal interstitium. * Predisposing factors: • D.M • Urinary tract obstruction • Females: due to short wide urethra • Congenital vesico-uretral reflux • Immunosuppression.
* Organism:E. coli (most common), staph, pseudomonas * Routes: • Ascending. • Haematogenous (rare).