Scleroderma: Symptoms, Diagnosis, and Management
Learn about different types of scleroderma, its symptoms, diagnosis, and treatment options. Scleroderma is a multisystem disease that affects various organs, including the skin, lungs, heart, and kidneys. Discover the natural history, clinical features, and complications associated with different subsets of scleroderma. Find out about the impact on patients' lives, including disability and special situations. This comprehensive guide aims to provide insights into managing scleroderma effectively.

Scleroderma: Symptoms, Diagnosis, and Management
E N D
Presentation Transcript
SCLERODERMA Virginia Steen, MD Professor of Medicine
Scleroderma • Localized Scleroderma • Morphea • Linear Scleroderma • En Coup de Sabre (Progressive Hemi-atrophy) • Pansclerotic, Deep subcutaneous
Linear Scleroderma Hyperpigmented, Muscle atrophy but normal strength Linear, single extremity
Linear Scleroderma Severe contractures, growth disturbances, atrophy
Systemic Sclerosis An uncommon disease 250/million population, 20 new cases/ million per year, about 80- 150,000 in US Age onset usually 30-50 years, rare under 10. Female 3-5: 1; Increased in African-Americans Multisystem disease - Raynauds, digital ulcers, arthritis, tendon inflammation, skin thickening, myopathy, gastrointestinal, lung, heart and kidney involvement Survival – decreased primarily from severe lung involvement, pulmonary fibrosis and pulmonary hypertension
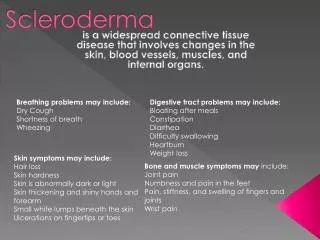
Diagnosis • Clinical diagnosis by Rheumatologist • Raynaud’s • Swollen fingers and/or skin thickening of hands/face • Esophageal symptoms-GERD. • Other organs- • Small intestines • Pulmonary Fibrosis • Pulmonary Hypertension • Cardiac or Kidney involvement
Laboratory Diagnosis • Laboratory - not required • Antibodies helpful for prognosis, but not necessary for diagnosis ( even ANA can be negative) • There can be false positives, particularly slightly positive tests • GI x-rays supportive but not required for diagnosis
Clinical features associated with limited and diffuse scleroderma Limited cutaneousDiffuse cutaneous Raynaud’s -1st symptom, Raynaud’s often delayed alone for many years Acute onset, a lot of Milder general symptoms constitutional symptoms Milder joint symptoms Arthralgias, carpal tunnel Tendon friction rubs Puffy FINGERs Swollen, puffy HANDs Limited skin thickening Early diffuse skin Anti-centromere antibody Anti-Scl 70 antibody Anti-RNA polymerase III
NATURAL HISTORY OF SCLERODERMA SUBSETS Contractures Renal crisis Myocardial failure 50 SKI N THICKNESS Pulmonary fibrosis 40 Diffuse scleroderma 30 20 Pulmonary hypertension Malabsorption Limited scleroderma 10 0 15 20 5 10 DISEASE DURATION (YEARS)
Evaluation of Skin Thickening Rodnan Skin Score 17 different sites- Score 0 to 3 Total 51 Limited - <12 Diffuse >12 Measuring skin thickness. Rodnan Skin Score Other Measures- Health Assessment Questionnaire Medsger Severity Scale (only research)
Joint and Tendon • Hand swelling, joint pain and stiffness- fingers, wrists, swelling/puffiness, other joints also • Contractures- hands, wrists, hips, shoulders, elbows. • Acroosteolysis- deformity causing loss of function • Tendon rubs- painful- hands, arms, ankles, knees
Gastrointestinal Involvement • Esophageal- trouble swallowing, heartburn, reflux, potential aspiration • Stomach –bloating, inability to eat full meals, need to eat small frequent meals • Small Intestine- malabsorption, diarrhea, pseudo obstruction, bacterial overgrowth, weight loss, need for hyperalimentation. • Large Intestine- constipation, rectal prolapse • Rectum- fecal incontinence
PULMONARY PROBLEMS IN SYSTEMIC SCLEROSIS • Pleurisy, pleural effusions, pleural scarring • Spontaneous pneumothorax (bronchiectasis) • Aspiration pneumonia • Malignancy-all cell types • BOOP • Interstitial fibrosis • Pulmonary vascular disease (PHT)
Pulmonary Fibrosis • Shortness of breath with activity • Fatigue with activity • Pulmonary function tests- Decreased FVC, TLC and DLCO, restrictive disease • CT scan of lung- scarring, honeycombing • Begins early in disease and progresses slowly or rapidly, major cause of death
Pulmonary Hypertension • Shortness of breath and fatigue with exercise • Occurs later in illness • More common in limited scleroderma • Low DLCO on PFTs, and high PAP on echo • Most common cause of death
Heart and Kidney • Less common but more serious • Heart- Pericarditis, pericardial effusion, cardiomyopathy, rhythm problems, heart failure • Kidney- Malignant hypertension, kidney failure, dialysis.
Disability in Limited Scleroderma • Usually after a long history of Raynaud’s, (unless digital ulcers) • Pain, fatigue, GI symptoms • Loss of hand function – digital ulcers, loss of mobility/dexterity, fine motion • Fatigue/shortness of breath- anemia, weight loss, GI, pulmonary fibrosis/hypertension.
Special Situations • Raynaud’s – can be disabling without ulcers, if job is outdoors, requires cold exposure (meat cutter) • Limited skin- can be disabling even without contractures if very swollen, late acroosteolysis, need for fine motion • GI –can be very disabling - with severe reflux, vomiting, difficulty swallowing, fatigue, inability to eat, weight loss
Disability in Diffuse Scleroderma • Early in Disease- mostly from progressive skin thickening, pain, fatigue, weight loss, contractures, digital ulcers. • Pulmonary fibrosis • Heart and Kidney
Special Consideration • Most diffuse scleroderma patients have enough problems that they are disabled. • While some diffuse scleroderma patients are able to continue working, it is usually because they are professionals and have a very flexible work situation.