Download
1 / 29
300 likes | 333 Views
Explore various respiratory infections affecting the upper and lower respiratory systems, including sinusitis, pharyngitis, pneumonia, and tuberculosis. Learn about symptoms, diagnostic methods, and treatments for each condition.

E N D
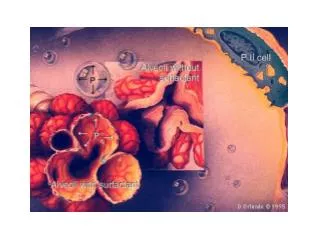
Introduction Respiratory system Serves as host for infectious diseases, although contains many layers of defense Warm, moist atmosphere facilitating microbacterial growth Site for constant inhalation of environmental particles 9-3
Upper Respiratory Infections • Includes • Sinusitis • Pharyngitis • Epiglottitis • Croup 9-4
Description Inflammation of hollow sinuses in nasal cavity Viral or bacterial Signs/Symptoms (S/S) (not limited to): nasal stuffiness and discharge; pain/pressure in face; if bacterial, yellow or green nasal discharge Diagnostic Observe for ten days to determine if self-limiting or if treatment required (Continues) Sinusitis 9-5
Treatment Oral decongestants Topical decongestants Nasal steroids Analgesics Antibiotics Sinusitis 9-6
Description Inflammation of pharynx and surrounding lymphatic tissue Viral or bacterial S/S (not limited to): sore throat; dysphagia; fever; white, mucosal patches Treatment: usually self-limiting; if bacterial, antibiotics Severe complications, if untreated Pharyngitis 9-7
Description Acute airway obstruction (airway emergency) Prevalent in children 2–6 years of age Abrupt onset (usually due to haemophilis influenzae Type B) Symptoms (4 Ds): distress (respiratory), drooling, dysphasia, dysphonia Treatment Maintain airway Antibiotic therapy Epiglottitis 9-8
Description Infection of laryngeal area, prevalent in children younger than 3 years of age Usually viral S/S: barking cough, stridor, may be afebrile Treatment: air humidification, administration of oxygen, nebulized epinephrine or corticosteroids Croup 9-9
Lower Respiratory Infections • Includes • Acute bronchitis • Acute bronchiolitis • Pneumonia • Tuberculosis 9-10
Description Affects bronchi; common in winter months Usually viral and may be self-limiting S/S: may progress from nonspecific symptoms (e.g., headache, sore throat) to thick bronchial secretions with productive cough; bilateral rhonchi and coarse crackles Treatment: symptomatic treatment, antibiotics (if bronchitis due to pertussis) Acute Bronchitis 9-11
Bronchiolitis Description Affects bronchioles, especially in infants 2–10 months of age; often in winter–spring months S/S (not limited to): restlessness, mild fever, noisy upper airway breathing, tachypnea Most common cause: RSV Treatment: antivirals, aerosolized drug using special nebulizer equipment (hood or mist tent) 9-12
Pneumonia • Many types • Community-acquired pneumonia • Atypical pneumonia • Viral pneumonia • Tracheobronchitis • HCAP, VAP, HAP • Aspiration pneumonia • Pneumocystis jiroveci (Continues) 9-13
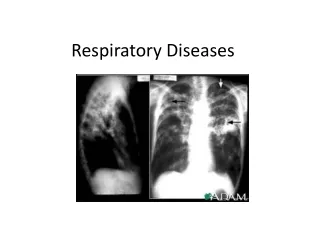
Pneumonia Description Causes: virus, bacteria, fungus, drugs or chemicals S/S (not limited to): leukocytosis, fever, rhonchi, dullness of percussion at site Diagnostic: chest x-ray and cultures of sputum and blood Assess respiratory function to determine need for hospitalization 9-14
CAP Description of infection is determined by prevalent pathogens, not geographical location Usual cause: Streptococcus pneumoniae Treatment Determined by such guidelines as local resistance patterns, clinical condition, chest x-ray results Recommended treatments are frequently updated Community-Acquired Pneumonia 9-15
Atypical Pneumonia • Description • Cause: organisms not detectable by gram stain, nor growth on standard cultural media • Organisms do not respond to antibiotics used to treat pneumonia • Often due to Mycoplasma pneumoniae, Legionella, Chlamydophila pneumoniae • Treatment • Empiric therapy 9-16
Viral Pneumonia • Description • Determined by molecular diagnostic methods, such as polymerase chain reaction (PCR) test • Must rule out bacterial cause • Bacteria and virus can coinfect • If bacterial, treat with antibiotics 9-17
Tracheobronchitis • Pneumonia-like infection caused by mechanical ventilation • S/S: fever, new/increased sputum production • Diagnostic: sputum sample from endotracheal tube for gram stain and culture • Treatment • Antibiotics (determined by local antibiotic susceptibility patterns) 9-18
HCAP, VAP, HAP • Health care–associated (HCAP), ventilator- associated (VAP), hospital-acquired (HAP) • Pneumonia related to exposure to/frequent contact with health care settings • Preventive measures: decrease aspiration by patients; prevent cross-contamination; disinfection/sterilization of respiratory devices; vaccines against certain infections; education of hospital staff and patients 9-19
Aspiration Pneumonia • Two types • Chemical • Exposure to stomach acid • Treatment: symptomatic therapy allowing lungs to heal • Bacterial • Due to aspiration of oropharyngeal organisms, or aerosol inhalation • Treatment: empiric antibiotic therapy 9-20
Pneumocystis jiroveci (Carinii) • Description • Due to defects in cell-mediated immunity (e.g., complications of HIV; organ or bone marrow transplantation; medications) • S/S (not limited to): asymptomatic (or) fever, cough, tachypnea, dyspnea • Diagnostic: ABGs • Treatment: specific IV or parenteral medications 9-21
Tuberculosis • Airborne, chronic disease due to Mycobacterium tuberculosis • Latent: inhaled droplet is encapsulated • Active: inhaled droplet (bacilli) escapes • S/S: asymptomatic (or) weight loss, fever, night sweats, bloody sputum • Diagnostic: Mantoux or PPD, testing of sputum specimen, chest x-ray (Continues) 9-22
Tuberculosis • Treatment • If latent • Preventive treatment (isoniazid 6–12 months) • If active • Medication regimen 6–24 months • Directly observed treatment (DOT) may be required due to noncompliance 9-23
Bioterrorism • Pulmonary irritants • Chlorine, phosgene • Biochemical reactions of irritants cause laryngospasm and pulmonary edema • Anthrax • Transmission: skin contact, inhalation • If inhaled, spores are transported to lymph system, germinate and produce toxins • Treatment: antibiotics (Continues) 9-24
Bioterrorism • Plague • Potential bioweapon, contagious • Transmission: close contact, aerosol • Treatment • If systemic: parenteral antibiotic therapy • Prophylaxis (post-exposure): oral antibiotics • Vaccine no longer available; discontinued in 1999 9-25
Avian Influenza (H5N1) • Carried in intestines of wild birds; transmitted to domestic birds, including poultry (cause of human exposure) • May be transmitted through touching contaminated surfaces • S/S noted after a 2- to 5-day incubation period include (not limited to) fever, cough, rhinorrhea, diarrhea, abdominal pain (Continues) 9-26
Avian Influenza (H5N1) • Symptoms may progress to acute respiratory distress syndrome • Treatment • Prophylaxis and supportive treatment • Antiviral medications • Includes treatment of anyone living with infected patient 9-27
Summary • Clinical presentation, diagnosis, treatment of respiratory system infections • Upper respiratory infections • Lower respiratory infections • Bioterrorism • Avian influenza (Continues) 9-28
Summary • Many upper respiratory tract infections due to viruses • Treating viral infections with antibiotics promotes bacterial resistance • Refer to text/tables for in-depth information 9-29