Download
1 / 35
370 likes | 857 Views
CLINICAL FEATURES EPIDEMIOLOGY LAB DIAGNOSIS PROPHYLAXIS TREATMENT k.vanya. Clinical features . Clinical features of B.anthracis:. Anthrax is a zoonotic disease. Anthrax “coal” ,comes from black colour of eschar

E N D
CLINICAL FEATURES EPIDEMIOLOGY LAB DIAGNOSIS PROPHYLAXIS TREATMENT k.vanya
Clinical features of B.anthracis: • Anthrax is a zoonotic disease. • Anthrax “coal” ,comes from black colour of eschar • Route of infection: ingestion / inhalation of spores /it may enter directly through skin. • Infective material: discharges from mouth , nose &rectum of infected animals. • The large no. of bacilli present in those discharges sporulate in soil and remain as source of infection. • Direct spread from animal to animal is rare.
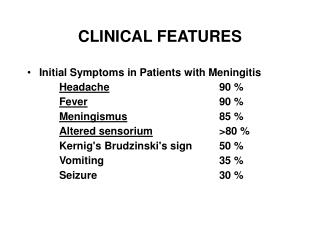
it causes fatal septicemia, but some times it is localized/resemble cutaneous diseases in humans. • acquired from animals directly / indirectly. • Based on clinical features, Anthrax is divided into 3 types cutaneous pulmonary intestinal • All these lead to fatal septicemia/meningitis
Cutaneous anthrax • Also called “hide porter’s disease”, as it is common in dock workers, • Route of infection: infection enter through abraded skin. • Also by shaving brushes made of animal hair • Usual sites: face,neck,hands,arms&back • Lesion starts as papule 1-3 days after infection • becomes vesicular (fluid clear/blood stained)
Malignant pustule: • The whole area congested, edematous & several satellite lesions filled with yellow fluid/serum arranged around central necrotic lesion which is covered by black eschar. • resolves spontaneously. Complications: 10-20% develop fatal septicemia/meningitis
Malignant pustule • Congested • Edematous • Satellite lesions
Pulmonary anthrax • Also called “wool sorter’s disease”. • Because it is common in wool factories. • Route of infection: due to inhalation of dust from infected wool. • More severe than others. • Complications: • hemorrhagic pneumonia (common) hemorrhagic meningitis(rare)
Intestinal anthrax • Rare • Mainly in primitive communities i.e. who eat dead bodies of animals died of anthrax. • Complication: violent enteritis with bloody diarrhea with high fatality rate
industrial • Based on occupation non-industrial • Industrial: such as meat packing/wool factories. • Non-industrial: associated with animals(butchers &farmers)
Rarely stomoxys calcitrans –biting insect transmit infection mechanically.
Epidemiology: • Rare in western countries • Large epidemics russia&zimbabwe (1978-80) • Recently visakha agency has outbreaks of cutaneous anthrax • Andhra –tamilnadu region • Cutaneous,meningoencephalitic infections
Specimens: • swab, fluid/pus from pustule-cutaneousanthrax • Sputum-pulmonary anthrax. • Blood-septicemia anthrax.
Microscopy: • Gram positive bacilli arranged in large chains.
Capsule --Clear halo around bacillus in Indian ink preparation
Direct flourescent antibody test: capsule specific staining for poly saccharide Ag • Mc fadyean’s reaction :Amorphous purple material – characteristic of B.anthracis. • Employed for presumptive diagnosis in animals
Culture : inoculated on nutrient agar incubate at 37 c for overnight. -medusa head colonies • Gelatin stab culture : inverted fir tree
Animal inoculation : white mouse / guinea pigs injected with exudate /culture • Animal dies in 48 hrs
Serology ( Ascoli Thermo Precipitin Test ): Tissues are ground up in saline and boiled for 5 mins and filtered. Then this extract layered over anti anthrax serum in a narrow tube. +ve case :ring of precipitate appears at junction of two liquids with in 5minutes. • mainly used for rapid diagnosis when sample received is putrid and viable bacilli less likely found
CDC(centers for disease control)guide lines: • Any large gram positive baciili with general morphology, cultural features of anthrax-non motile, on hemolytic on blood agar,catalase positive given presumptive report as anthrax. • Initial confirmation-lysis by gamma phage,DFA test. • Further confirmation:PCR test
Other methods : • Polymerase chain reaction : used for conformation of anthrax bacilli. • ELISA assay for antigen detection • X-ray and CT scan • Lysis by gamma phage
PROPHYLAXIS: General methods : • improvement of factory hygiene • proper sterilization of animal products , carcasses of animals suspected to have anthrax are buried deep in lime.
Active immunization • Spore is common infective form • Sterne vaccine contains spores of non capsulated avirulent mutant strain • Animal is protected for a year with single injection of spore vaccine • Extensively used in animals • Not safe for human use
Contd…. • Alum precipitated toxoid prepared from protective antigens used in persons occupationally exposed to anthrax infection. • Safe and effective in humans • Given in 3 doses IM at intervals of 6 weeks
Treatment: • Before 2001, 1st line of treatment was penicillin G • Stopped for fear of genetically engineered resistant strains • 60 day course of antibiotics • Ciprofloxacin • fluoroquinolone • 500 mg tablet every 12h or 400 mg IV every 12h • Inhibits DNA synthesis • Doxycycline • 6-deoxy-tetracycline • 100 mg tablet every 12h or 100 mg IV every 12h • Inhibits protein synthesis
For inhalational, need another antimicrobial agent • clindamycin • rifampin • chloramphenicol • Anthrax infection gives permanent immunity&2nd attacks are rare.