Download
1 / 66
710 likes | 1.84k Views
Diverticulitis. Sandra J. Beck, M.D., F.A.C.S., F.A.S.C.R.S Associate Professor of Surgery University of Kentucky Grand Round February 9, 2011. Objective: To answer frequently asked Questions regarding diverticulitis.

E N D
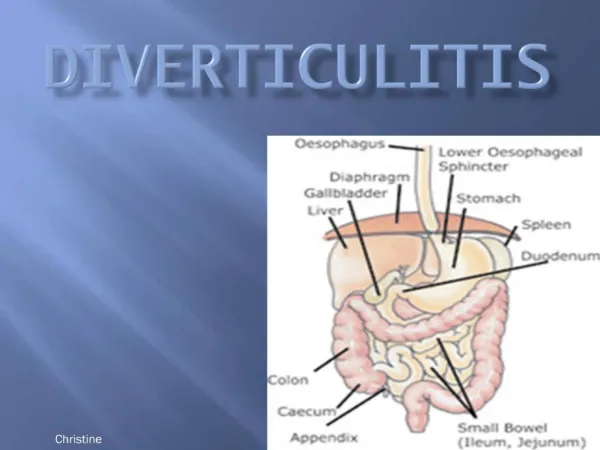
Diverticulitis Sandra J. Beck, M.D., F.A.C.S., F.A.S.C.R.S Associate Professor of Surgery University of Kentucky Grand Round February 9, 2011
Objective: To answer frequently asked Questions regarding diverticulitis • Does one have to avoid seeds nuts and popcorn if they have diverticulitis/diverticulosis? • When do you operate on diverticulitis? • Do all young patients (age < 50) require sigmoid colon resection?
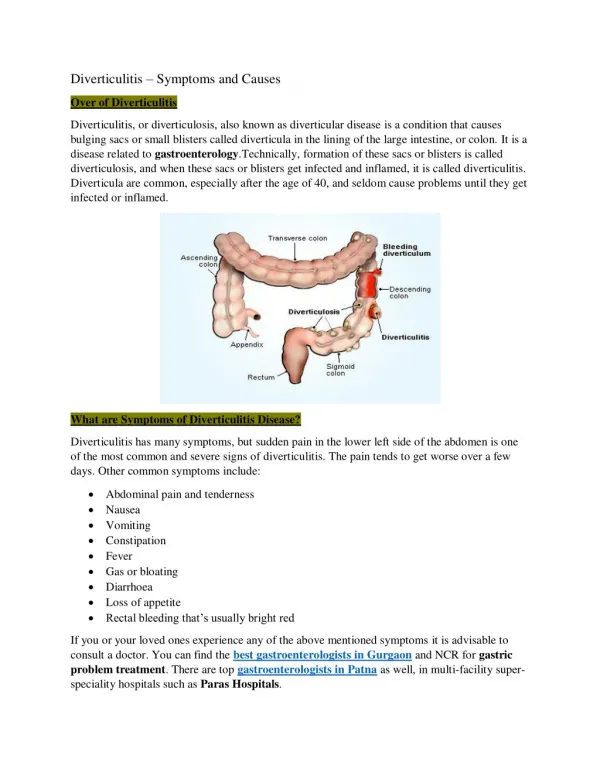
Etiology • Age – In the United States • 1/3 by age 60 • 2/3 by age 85 • Obesity • Diet – Western diet • Low fiber • High meat consumption • High sugar consumption • Distribution – more common in industrialized countries
Effect of the Industrial Revolution • No pathologic specimens in European museums or case reports of diverticulitis or diverticulosis prior to Industrial Revolution (~1750-1850)
Effect of the Industrial Revolution • Process of roller-milling wheat lead to decrease in fiber consumption • Increased consumption of meat and sugars by the general population • 25 year lag between roller-milling and the first cases of diverticulitis
Theories • 1920 British Journal of Medicine – C.H. Whilley, Consulting Surgeon • “I feel sure it would be illuminatingto note in all cases the particular type and build and temperament of the patients, as well as any temporarycondition of mental worry or powerful emotional disturbance. I haveno doubt of the very close connection between depressingemotion and pathologicalconditions of the largeintestine.”
Theories • 1926 British Journal of Medicine – R Davies-Colley • Subperitoneal fat weakens the muscular layer of the colon and then the fat becomes infected by the colonic contents. This infected fat then leads to weakening in the adjacent fat and inflammation results.
Theories Direct Trauma – proposed in 1960’s • Fecal matter (i.e. seed husk) causes direct trauma to the wall of the colon and incites inflammation • Weakness develops at the site of trauma and a diverticulum forms • Continued trauma and fecal matter inspissated within the diverticulum leads to diverticulitis
Theories Increased intraluminal pressure • Current theory based on epidemiological studies • Decrease in fiber in the diet • Hypertrophy of the colonic wall • Increase pressure to propel stool through the colon Fiber rich diet – sigmoid pressure = atmospheric Low fiber diet – sigmoid pressure = 90mmHg
Who Cares? – Popular Media • When Frasier is asked to endorse a brand of nuts on the popular TV show “Frasier” he says “Well, for one thing I don't like them, and they're sixty percent fat, they're laced with salt and they wreak havoc with my diverticulitis.”
Can we eat Seeds, Nuts and Popcorn? • Recommendation to avoid seeds, nuts and popcorn was a result of the theory from the 1960’s • Data? • 48% of colon and rectal surgeons still advise patient’s to avoid these foods • Nursing textbooks still follow these recommendations
Can we eat Seeds, Nuts and Popcorn? • Currently epidemiologic data supports the intraluminal pressure model of diverticulosis • However, the avoidance of seeds, nuts and popcorn persists
Can we eat Seeds, Nuts and Popcorn? • JAMA August 2008 • “Nut, Corn and Popcorn Consumption and the Incidence of Diverticular Disease” • Health Professionals Follow-up Study • Cohort of US men (51,529) followed prospectively from 1986 – 2004 • Follow diet, life style and medical history with biennially questionaire • 90% mean followup
Can we eat Seeds, Nuts and Popcorn? • Supplemental questionairre sent to 47,228 (after exclusions) men in 2004 • Looked at nut, corn and popcorn consumption and symptomatic diverticulitis • Conclusion: Nut, corn and popcorn consumption did not increase the risk of diverticulosis or diverticular complications • Inverse associations between nut and popcorn consumption and the risk of diverticulitis in patient’s who consumed them >2x/week
http://www.lifelongfitnessalliance.org/step-it-up/Fiber%20Content.pdfhttp://www.wehealny.org/healthinfo/dietaryfiber/fibercontentchart.htmlhttp://www.lifelongfitnessalliance.org/step-it-up/Fiber%20Content.pdfhttp://www.wehealny.org/healthinfo/dietaryfiber/fibercontentchart.html Nuts popcorn • 2.5g fiber per 1 oz • Vitamin E • ↓CRP and IL-6 levels • Rich in Zinc and Magnesium • Anti-inflammatory properties • 3.6g fiber per 3cup • Lutein – micronutrient with anti-inflammatory and chemoproctective properties
Fiber • Non-soluble and Soluble Fiber has several component non-starch polysaccharides • Lignin – non-carbohydrate component that is not fermented, attracts water, produces bulk, water insoluble, nuts and seeds • Celluloses – found in leafy vegetable, partially fermented • Fruit pectins – completely fermented, slow transit time, supply butyrate (main fuel of colonic epithelial cells), considered water soluble, psyllium, flax seed
Surgical Therapy of Diverticulitis “It depends”
Surgical Therapy of Diverticulitis • Clinical presentation • CT scan or other diagnostic tests • Colonoscopy • Complications • Fistula • Abscess • Peritonitis • Stricture
Clinical Presentation • Symptoms • Fever and/or chills • Left lower quadrant or lower abdominal pain • Change in bowel habits • Urinary symptoms including dysuria or pneumaturia • Presence of localized or generalized peritonitis • Sepsis • Elevated WBC count
Diagnostic Testing • CT Scan with contrast – diagnostic test of choice • Reliably shows the segment of bowel and the extent of disease • Identifies abscess and fistula formation • Reveals sympathetic involvement of adjacent organs such as the small bowel, bladder and abdominal wall • Can be used to guide percutaneous drainage • Can be used to classify severity of diverticulitis
CT classification or grading • Modified Hinchey Staging – Originally based on clinical findings at surgery • Stage 0: LLQ pain, elevated WBC, fever, no confirmation by imaging or surgery • Stage Ia: Confined pericolic inflammation or phlegmon • Stage Ib: Confined percolic abscess • Stage II: Pelvic, distant intraabdominal or retro-peritoneal abscess • Stage III: Generalized purulent peritonitis • Stage IV: Generalized feculent peritonitis
Classification of Diverticulitis Umcomplicated Complicated • Pain • Fever • Small pericolic abscess <2cm • Generally Stage 0 or Ia • Free intraperitoneal perforation • Large pericolic abscess or distant intra-abdominal or retroperitoneal abscess • Fistula • Stricture • Sepsis • Obstruction
Stage 0 • Often seen by Primary Care Doctor, GI or Emergency Department • Generally treated with Oral antibiotics • Cipro/Flagyl • Augmentin • Low residue diet initially • High fiber diet once symptoms resolve • Interval colonoscopy
Follow up of Stage 0 and Ia • Careful history regarding prior attacks including number, frequency, and severity • Interval Colonoscopy to rule out malignancy • High fiber diet • <25% will have second attack • Risk of third attack >50% after second attack • Laparoscopic approach in patients with multiple attacks
Stage III and IVComplicated Diverticulitis • Can be difficult to distinguish on CT Scan or clinically • Generalized or Localized Peritonitis • Sepsis • Fever • Elevated WBC
Stage III and IVComplicated Diverticulitis • Usually require emergent operative intervention • Hartman’s Procedure (1921) Colostomy with closure of distal bowel • Primary anastomosis with diverting loop ileostomy in select cases • Laparoscopic lavage with drainage and interval sigmoid colectomy
Stage III or IVComplicated Diverticulitis • Requires a second operation to restore intestinal continuity • High percentage of patients never have them reversed (25-70%) • Morbidity associated with stomas • Change in body image • Difficulty with stomal pouching • Peristomal hernia • Stomal retraction • Stomal prolapse
Stage Ib or II • Percutaneous drainage if possible • Transrectal drainage of pelvic abscess • IV antibiotic • Close clinical observation
Obstruction or Ileus may be indication for early surgical indication • May indicate inflammation of adjacent innocent small bowel
Ileus Bowel in right lower quadrant is dilated with air-fluid levels
Stage Ib or IIComplicated Diverticulitis • Close follow up to assure resolution of symptoms and monitor for recurrence • Interval colonoscopy to rule out malignancy • Segmental resection with primary anastomosis 4-6 weeks after episode • Laparoscopic approach (straight or hand assist) often successful • Risk of recurrence if managed conservatively secondary to complications of diverticulitis (abscess, stricture or fistula)
Laparoscopic Port Placement 5mm 5mm camera camera 5mm 5mm 12mm Extraction site Hand port Straight Laparoscopic Hand Assist
Other Complications of Diverticulosis Fistula and Stricture
Colonic FistulaComplicated Diverticulitis • Colo-cutaneous fistula • May be a consequence of percutaneous drainage of pericolicabsces • Colo-vesicle fistula • 50% of patients will not remember having diverticulitis • Men > Women • Pneumaturia, fecaluria, frequent UTI’s • Colo-vaginal fistula • Generally seen in post hysterectomy female • Sigmoid adhesions to the pelvis
Colonic FistulaComplicated Diverticulitis • Rarely a cause for emergent surgery • Patient often improves with fistula formation • IV antibiotics • Await decrease in inflammation
Colonic FistulaComplicated Diverticulitis • Diagnosis is largely based on history and physical • CT Scan may show air in the bladder with adjacent colonic thickening • Vaginoscopy will demonstrate stool in the vault • Cystoscopy – bullous edema and cystitis
Colonic FistulaComplicated Diverticulitis • Resection of the diseased segment of bowel • Preoperative Colonoscopy and Cystoscopy to rule out malignancy • Intraoperative ureteral stenting • Omental pedicle graft to separate colonic anastomosis from the bladder repair • Consider proximal diverting loop ileostomy to avoid Hartman’s procedure as redo-pelvic surgery will likely be more difficult
Colonic StrictureComplicated Diverticulitis • Usually due to adhesion formation or as a result of recurrent inflammation and scarring • Often difficult to distinguish from Crohn’s disease or Carcinoma • May be asymptomatic and identified at the time of colonoscopy • Diagnosis may be accomplished with Barium enema • If diagnostic uncertainty then surgical resection is recommended
Do all young patients (age < 50) require sigmoid colon resection?
Do all young patients (age < 50) require sigmoid colon resection? • Natural history of diverticular disease seemed to suggests that it behaves in a more virulent manner • More severe first attack with more patients having complicated diverticulitis at the time of first episode • Historically lead to the recommendation that sigmoid resection be performed after the first episode • 10-25% of diverticulitis patient <50 years old