Download
1 / 18
190 likes | 542 Views
Birth Injuries-Excluding Scalp and Intracranial Injuries. Adapted from a presentation by Vandana Nayal. Skull fractures. Bones of the skull are less mineralized at birth and thus more compressible. Follow repeated forceful contact of the fetal skull against the maternal pelvis

E N D
Birth Injuries-Excluding Scalp and Intracranial Injuries Adapted from a presentation by Vandana Nayal
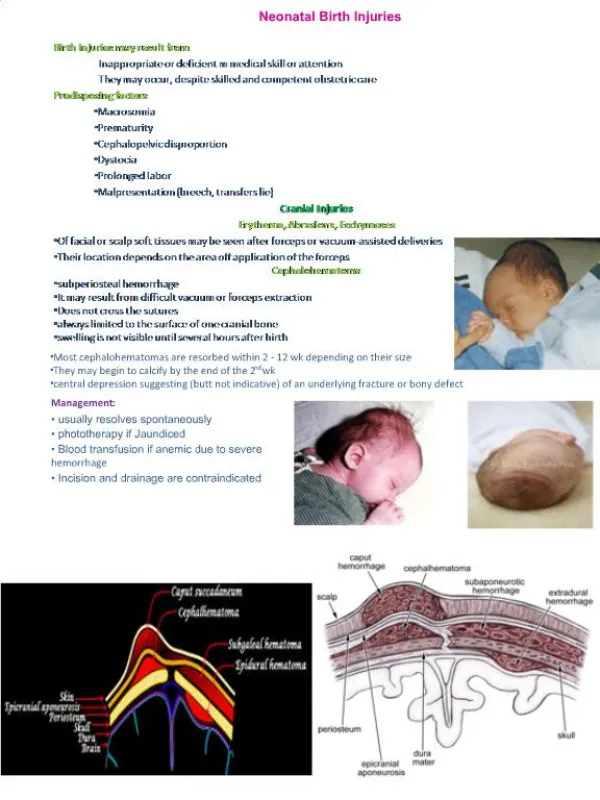
Skull fractures • Bones of the skull are less mineralized at birth and thus more compressible. • Follow repeated forceful contact of the fetal skull against the maternal pelvis • Linear fractures of the skull are accompanied by soft tissue changes and cephalhematoma • Depressed fractures are visible palpable indentations in the smooth contour of the skull( ping-pong) ball
Prognosis • Simple fractures heal without sequelae • Leptomeningeal cyst may develop, if detected early, cyst can be excised successfully and brain atrophy prevented • Repeat radiographs within 2-3 months to detect early widening of the fracture line
Facial nerve palsy • Prolonged 2nd stage and midforceps delivery • Central paralysis- limited to lower 1/2 or 2/3 of the contralateral side • Peripheral-entire side of the face • Persistently open eye on the affected side
Vocal cord paralysis • Uncommon injury, unilateral- symptom free or hoarseness with mild inspiratory stridor or bilateral-stridor, left more common than right • Unilateral- gentle handling and frequent small feedings, usually resolves within 6 wks • Bilateral is caused by hypoxia or hemorrhage into the brain stem • Bilateral-immediate intubation, tracheostomy required in most patients.
Fracture of the clavicle • Complete and some greenstick fractures may be apparent shortly after birth. Obvious callus at 7-10 days of age • Movement of the arm may be affected • Pain subsides in 7-10 days
Brachial palsy • Erb-Duchenne- C5+ C6 –upper arm paralysis,Moro, biceps and radial reflexes are absent, grasp reflex is intact, ipsilateral phrenic nerve injury with respiratory distress • Klumpke-lower arm paralysis-C8+T1-rare-intrinsic muscles of the hand and the long flexors of the wrist and fingers affected, grasp reflex is absent and tendon reflexes are present, ipsilateral Horner, delayed pigmentation of the iris- sensory deficit-ulnar • Paralysis of the entire arm- all reflexes absent,flaccid, sensory deficit up to shoulder
Eval and Therapy • Thorough physical-palpate sternomastoid, fractures of clavicle, humerus or ribs • Abdominal asymmetry- indicate paralysis of hemidiaphragm, ocular asymmetry- Horner syndrome • CT, MRI or myelography for avulsions • Electromyography is unreliable in predicting extent of damage • Exercises involving shoulder rotation,elbow flexion and extension, wrist flexion, thumb abduction,adduction and opposition
Treatment • Infant evaluated every month and if no improvement in deltoid, biceps and triceps function occurs by 3rd month, good outcome without surgery is not likely • Primary brachial plexus exploration during the fourth month • Exploration,evaluation and repair of the injury has resulted in 90% of patients having useful function above the elbow • Function below the elbow has resulted in 50% to 70% recovery
Phrenic nerve paralysis • Difficult breech delivery • Recurrent episodes of cyanosis, irregular and labored respirations • Breathing is almost completely thoracic, no bulging of the abdomen, excursions on the involved side are ineffectual • Areas of atelectasis appear bilaterally • US shows abnormal motion of the diaphragm • Fluoroscopy only for the equivocal case
Treatment • O2 for cyanosis or hypoxemia, IV fluids, gavage feedings, antibiotics are indicated if pneumonia occurs • If bilateral, assisted ventilation shortly after delivery • Infants who did not recover diaphragmatic function within 30 days did not demonstrate recovery-disruption of the phrenic nerve • Candidates for plication of the diaphragm early in the 2nd month of life
Injuries to spine and spinal cord • Result from breech deliveries, brow and face presentations • High cervical-Stillborn, respiratory depression, shock, hypothermia • Upper or mid-cervical region-flaccidity and immobility of the lower limbs, cardiac function is strong, urinary retention may be the first symptom, paralysis of the abdominal wall, intercostal muscles may be affected , sensation is absent over the lower half of the body, absent DTR, constipation, brachial plexus involved in 20%
Spinal cord injuries • 3rd group-C7-T1- survive for long periods, transient paraplegia, skin is dry and scaly, muscle atrophy, contractures and bony deformities, bladder distention and constant dribbling followed by paraplegia in flexion, spontaneous micturition, mass reflex and profuse sweating over the involved part of the body • 4th group- partial spinal cord injury and CVA. subtle neurologic signs of spasticity- cerebral palsy
Treatment • Infants affected at birth require basic resuscitative measures • In case of vertebral fracture-immediate neurosurgical consultation for reduction and relief of cord compression, followed by appropriate immobilization • Position of paralyzed parts should be changed every 2 hrs, indwelling urinary catheter should be inserted • Urology consult
Injuries to intra-abdominal organs • Rupture of the liver- large infants, IDM,breech • May appear normal from 1-3 days of life, any infant with shock, abdominal distension, pallor, anemia, and irritability with no evidence of blood loss • Crit and hgb stable initially, then sudden circulatory collapse, with rupture of the hematoma through the capsule • Abdomen is rigid, bluish discoloration of the overlying skin. CT scan may help in diagnosing subcapsular hematoma
Treatment • Prompt transfusion of prbcs and correction of coagulation disorder • Laparotomy with evacuation of the hematoma and repair of any lacerations • Any fragmented, devitalized liver tissue should be removed • Blood transfusion and the tamponade of intra-abdominal pressure might be adequate therapy in some infants
Rupture of the spleen • Large infants in breech position, erythroblastosis, congenital syphilis • Underlying clotting defect • Clinical signs of hemoperitoneum and blood loss • Left upper quadrant mass and medial displacement of the gastric bubble • Packed rbc’s and exploratory laparotomy • Attempt to repair and preserve the spleen
Adrenal hemorrhage • Increased size and vascularity at birth • Macrosomic, IDM, cong syphilis, neuroblastoma, hemorrhagic disease • Fever, tachypnea, cyanosis, mass in flank and purpura • Adrenal insufficiency, poor feeding, vomiting, uremia, convulsions and shock • US- initially solid appearance then cystic • Blood , IVF and corticosteroids • Laparotomy, evacuation of clots if extends to peritoneal cavity