Download
1 / 56
580 likes | 751 Views
TRICHINELLA SPIRALIS. Intestinal helminths, and other tissue Nematode Intestinal infection ,in which adult worms are found in the mucosa of the intestine and encysment of larvae are found in the muscle.

E N D
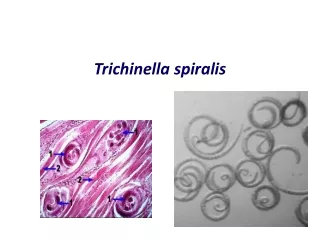
TRICHINELLA SPIRALIS • Intestinal helminths, and other tissue Nematode • Intestinal infection ,in which adult worms are found in the mucosa of the intestine and encysment of larvae are found in the muscle. . Parasite of carnivorous mammals, especially common in rats and in swine fed uncooked. • ONE SPECIES, Trichinella spiralis, IS A PARASITE OF MAN. • ANOTHER SPECIESES : * Trichinella nativa ( Kutub ) * Trichinella nelsoni ( Africa ) * Trichinella britovi ( Europe ) * Trichinella pseudospiralis
Trichinella spiralis MORPHOLOGY • THE CAUDAL END OF THE FEMALE IS BLUNTLY ROUNDED, WHILE THE MALE IS CURVED AND HAS A SINGLE SPICULE. • THE FEMALE SINGLE OVARY AND THE VULVA IS NEAR THE LEVEL OF THE BASE OF THE ESOPHAGUS. • . THE FEMALES ARE VIVIPAROUS • THE ADULT INHABIT IN THE INTESTINE AND THE LARVAE IN THE MUSCLE OF MAMMALS. • The adult is a small worm with a slender anterior end. • THE MALE • From 1.4 to 1.5 mm long and 0.04 mm broad. • The cloaca is at the ventrally curved posterior end between two lobular caudal appendages which serve during copulation. picture
Trichinella spiralis MORPHOLOGY The adult is a small worm with a slender anterior end. • THE FEMALE • From 3 to 4 mm long and 0.06 mm broad. • The vulva is in the anterior fifth of the body, and a single ovary is near the bluntly rounded caudal end. • The small terminal mouth is nonpapillae and leads into the pharyngeal esophagus. picture
Trichinella spiralis MORPHOLOGY • THE LARVA • With a spearlike burrowing tip at its tapering anterior end measure 80 to 120 by 5 to 6 at birth and grows but little until it has entered a muscle fiber where it attains a size of 800 to 1,300 by 35 to 40 . • The mature larva has a digestive tract similar to that of the adult, and while the reproductive organs are not fully developed, it is often possible to differentiate the sexes.
Trichinella spiralis REPRODUCTION Each viviparous female produces from 1350 to 1500 larvae. • VIABILITY • Endcysted larvae are killed at temperature above 550C. • The infectivity is reduced by refrigeration at 50C for 27 hours. • By exposure to pepsin for 12 hours. • Irradiation of the larvae inhibits the reproductive capacity of the ensuing adult worms. • Storage at – 15 C for 20 days or – 30 C for 6 days will kill endcysted larvae.
TRICHINELLA SPIRALIS HOSTS • Trichinella spiralis is found chiefly in : • Man • Hogs • Rats • Bears • Foxes • Dogs • Cats, but any carnivorous or omnivorous animal may be infected.
TRICHINELLIASIS ETIOLOGY: Trichina spiralis another name isTrichinella spiralis hominis DISEASES : TRICHINOSIS; TRICHINIASIS; TRICHINELLIASIS • HISTORY : • Trichinella spiralis is Non Soil Transmitted Helminth and tissue Nematode • The encysted larval worm in man was first noted in Germany in 1822 and later in England in 1828 and 1833. • The larval worm was described in 1835 named it Trichina spiralis. • T spiralis is cosmopolitan and high pathogenecity • T pseudospiralis , cosmopolitan, does not encyst, infectious to birds and pathogenicity in humans not well characterized
TRICHINELLIASIS GEOGRAPHIC DISTRIBUTION • Cosmopolitan. It occurs more frequently in the Northern Hemisphere and less frequently in the tropic. • It is particularly prevalent in countries where pork is eaten raw or insufficiently cooked, and thus is rare in Moslem and Hindu.In Indonesia especially in Bali. • Survey in Jaya Wijaya Papua Indonesia indicate that infections with Trichinella sp in pigs are present.
Trichinelliasis LIFE CYCLE • The same animal acts as both final and intermediate host, harboring the adult parasite temporarily and the larva for a long period. • In order to complete the life cycle, flesh containing the encysted larvae must be ingested by another host. picture
Trichinelliasis LIFE CYCLE • The adult worms are attached or hidden in the intestinal mucosa. • Found in the small intestine from the duodenum to the ileocecal valve and sometimes in the cecum and first portions of the colon. • When infective stage are ingested by humans, usually in raw or poorly cooked pork ,they pass to the upper small intestine, where the capsules are digested and the larvae released in a few hours by the action of digestive juice.The liberated larvae immediately invade the intestinal mucosa. • They rapidly penetrate into the epithelium of the duodenal and jejunal mucosa • The amount of damage to the intestinal lining is depend on the number of invaiding organisms and the time and number of previous exposures.
Trichinelliasis LIFE CYCLE * In 18 to 24 hours may be differentiated in male and female * Within two days the worm reach sexual maturity and mate in the small intestine * After copulation gravid female increases in size and in about 48 hours, burrows deeply into the mucosa of the intestinal villi from the duodenum to the caecum and even in the large intestine in heavy infections * About the fifth day female worm begins to deposit larvae into the mucosa and sometimes directly into the lymphatics from which they reach the thoracic duct and enter the blood stream and the larvae are carried to all parts of the body. .
Trichinelliasis DEVELOPMENTAL CYCLE • * After passing through the hepatic and pulmonary • filters the larvae are carried to all parts of the body. * Burrow into the muscle fiber, and capable of encysting and developing only in streated muscle
Trichinelliasis DEVELOPMENTAL CYCLE • Larvae have been found in the skeletal muscles, lungs, myocardium, brain, retina, intestine, bone marrow, blood, cerebrospinal fluid, various serous cavities and other tissues. • They have a predilection and usually only develop in striated muscles. • They rarely settle in other tissues and if so they soon disintegrated and are absorbed.
Trichinelliasis DEVELOPMENTAL CYCLE • Larvae have been detected in myocardial lesions as early as the fifth day (Dunlap and Weller, 1934). • The invasion of the muscle usually begins from 6 to 9 days after infection. • The larva burrows into the muscle fibers by means of a spear-shaped apparatus at its anterior end. • The larva grows in the long axis of the muscle fiber; it begins to coil for encystment by the seventeenth day, when it has become resistant to pepsin and capable of infecting a new host.
Trichinelliasis DEVELOPMENTAL CYCLE • It attains its maximal size about the 20th day. • Encapsulation begins about the twenty-first day and the larva becomes encapsulated in a lemon-shaped capsule of sarcolemmous origin, 0.4 by 0.25 mm. • The cyst rarely contains more than one larva. • The permanent capsule is completed in about 3 months. • Calcification begin as early as 6 months or within 2 years • Calcification is usually completed within 18 months, but the encysted have may remain viable for long periods; a duration of 11 years in the hog and 31 years in man has been recorded. • Adult female dies after passing her larvae and then is digested or passed out of the intestine.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY * Can be occurred because of : - The intestinal lessions caused by the adult worm - The presence of the larvae in the striated muscles and vital organs. -The reaction of the host to their activities, antigenic products, and possible toxic reaction * In 3 to 4 days after invasion of the larvae ,the muscle fibers increase in size, and become edematous . * The nuclei increased in size and number *The adjacent muscle fibers undergo hydrophic degeneration and hyaline necrosis.
Trichinella spiralis TRICHINELLIASIS • PATHOLOGY • These organs show widespread focal necrosis and an intense eosinophilic reaction. • Evidently the reaction of the host to the parasite rather than the effect of the parasite on the host is responsible for the clinical manifestations. • The clinical picture suggest that the damaging factors are the result of an antigen-antibody reaction or have a toxic or allergic background.
Trichinella spiralis TRICHINELLIASIS • PATHOLOGY • * The distribution of larvae in mild and severe infections follows the same pattern with heaviest concentration in the skeletal muscle of the forearm, intercostals and tongue, and no larvae in the viscera, brain, or circulatory system. • * The lodgement of the migrating larvae in the capillaries and perivascular sites throughout the body produces an inflammatory cellular reaction, necrosis, edema, hyperemia, petechiae, and infarction.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY The pathologic changes in man involve many organs : * Gastrointestinal tract * Lungs * Skeletal muscles * Heart * Central Nervous System * Miscellaneous organs
Trichinella spiralis TRICHINOSIS PATHOLOGY IN MAN • Gastrointestinal tract • In man who rarely dies in less than three weeks, the early gastro-intestinal changes are not significant. • The activities of the adult worms and larvae may produce a catarrhal enteritis with hyperemia, petechial hemorrhages, edema and occasionally slight ulceration of the mucosa. • The hyperplastic mesenteric lymph nodes are hyperemic or gelatinous. • The accompanying symptoms of gastro-intestinal irritation, edema, and urticaria are usually attributed to the activities or proteic products of the worms, although the possibility of a toxic secretion has been suggested.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Lungs • During passage through the lungs some larvae may leave the pulmonary capillaries and produce petechiae and small foci of pneumonitis. • Hemorrhages, nodular consolidations. • Blood-tinged pleural effusions, small hemorrhagic foci, pulmonary edema and infiltration, bronchitis, bronchopneumonia, and pulmonary infarction and embolism have been observed in man.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Striated muscles • The muscle fibers, particularly in the tendon of the muscle, are invaded by the larvae. • Three or four days after the invasion, the muscle fibers increase in size, become edematous, develop a spindle shape, lose their cross striations and undergo basophilic degeneration. • The nuclei increase markedly in number and size, become oval rather than rod-shaped, stain less intensely, and migrate from their normal position beneath the sarcolemma to the interior of the muscle fiber.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • The metabolism of the muscle is somewhat altered, with a decrease in glycogen and an increase in protein and lactic acid. • There is an acute interstitial inflammation about the parasitized muscle fiber, which reaches its peak in five or six weeks, with edematous swelling, and cellular infiltration of polymorphonuclear neutrophils, eosinophils, lymphocytes, and at times foreign body giant cells. • Later the inflammation and edema dissapear, but the adjacent muscle fibers undergo hydropic degeneration and hyaline necrosis.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • The larva is gradually enclosed in a lemon-shaped cyst, which is composed of an inner mantle of basophilic degenerative muscle plus epithelioid cells and fibroblasts and an outer hyaline capsule derived from the sarcolemma. • The latter is probably the expression of an antigen-antibody reaction. • The permanent capsule is completed in about three months.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Heart • Exudative changes in the heart are caused by the migrating larvae, which although they never encyst in the myocardium, are either killed there or enter the general circulation. • Macroscopically the heart is soft, and reddish brown, and sometimes the pericardium is injected and contains increased fluid.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • The myocardium and endocardium show mild edema, passive hyperemia, petechial hemorrhages, and numerous focal areas of interstitial infiltration with neutrophilic and eosinophilic leukocytes, lymphocytes, macrophages, plasma cells, and at times fragmentation, fatty degenartion, and necrosis of the muscle fibers. • These lesions, which are the result of a nonspecific reaction to the migrating larvae, account for the transitory cardiac symptoms in trichinosis and apparently do not represent permanent changes.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Central Nervous System • Lesions of the central nervous system are fairly common but inconstant. • They may represent an acute nonsuppurative meningitis with edematous hyperemic meninges, or may serious focal cerebral damage. • Larvae have been found in the spinal fluid, which shows increased pressure.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Eyes • The eyes frequently exhibit a characteristis chemosis of the bulbar conjuctiva with round-cell infiltration, necrosis, edema, and accumulation. • In the choroid there is a marked accumulation of leukocytes and a proliferation of the endothelial cells of the capillary walls, which frequently are thickened, hyalinized, and dilated.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Miscellaneous organs • The larvae may invade the lungs, pleura, pancreas, gallbladder, kidney, and other organs, producing local inflammation and edema. • The heart, kidneys, and liver may show fatty degeneration. There may be hyperplasia of the bone marrow with an increase in eosinophils.
Trichinella spiralis TRICHINELLIASIS PATHOLOGY IN MAN • Laboratory Examination : • The leukocyte count may range from 4.000 to 34.000 but generally is from 7.000 t0 17.000. • The percentage of eosinophils starts to increase in the second week, and after the third week usually runs from 15 to 40 % but may be as high as 89%. • It gradually declines to about 5 % in six months and to normal in one year, but sometimes remains elevates for years.
Trichinella spiralis TRICHINELLIASIS SYMPTOMATOLOGY • Five factors determine the variability of clinical symptoms: • The number of worms • The size and age of the patient • The tissues invaded • The general resistance of the patient • The presence of concominant pathological condition.
Trichinella spiralis TRICHINELLIASIS SYMPTOMATOLOGY • The essential symptoms probably arise from the toxemia and activities of the parasite, but some workers consider them allergic. • The disease is commonly divided into three cllinical phases corresponding to the periods of : • Intestinal invasion by adult worms • Migration of the larvae • Encystment and repair. • The incubation period varies from 2 to 30 days, but usually ranges from 5 to 17 days.
Trichinella spiralis TRICHINELLIASIS SYMPTOMATOLOGY • During the period of invasion the encysted larvae and adult worms may produce symptoms of gastro-intestinal irritation and intoxication: nausea, vomiting, and a watery diarrhea without blood or mucus. • The early gastro-intestinal phase, resulting from the mechanical or toxic action of the worms, is often overlooked. • Fever, profuse sweating, rapid cardiac and respiratory rates, edema of the face, and urticarial manifestation, also occur.
Trichinella spiralis TRICHINELLIASIS SYMPTOMATOLOGY • At the start of migration, some 5 days after infection, the previous symptoms recur from toxic effect of the larvae. • The fever, rarely over 1040F and frequently below 990F, is typhoidal in type; there is edema of the face and eyelids, headache, and sometimes delirium. • Respiratory, ocular, and cardiac symptoms and more rarely a maculopapular erythema or petechial rash may appear. • The second stage usually lasts from 8 to 15 days, but because of the continuous production of larvae the symptoms of the second and third stages overlap so as to produce a confusing clinical picture.
Trichinella spiralis TRICHINELLIASIS SYMPTOMATOLOGY • When the muscles are invaded, a marked interstitial myositis is established, producing rheumatoid symptoms with muscle tenderness and spasm. • After the third week the leading symptoms in order of prevalence are : eosinophilia, edema chiefly orbital, muscular pain, and tenderness, headache, fever, generqal weakness, joint pain, and rarely hyperethesia. • In severe case patients may show cachexia. • The cardiac symptoms that arise from the pathological changes produced by the larvae in the myocardium during their migration are usually transient.
Trichinella spiralis TRICHINELLIOSIS SYMPTOMATOLOGY • Extensive myocardial damage, may result migration and death. • The symptoms are a feeble or dicrotic pulse, suffled heart sounds, an apical systolic murmur, tachycardia, palpitation, hypotension, and edema. • About one sixth of the patients show electrocardiographic changes; evidence of myocardial damage by the slurring of the peak of the Q.R.S. complex, premature contractions the prolongation of the P-R interval and flattening or inversion of the T waves.
Trichinella spiralis Correlation of Clinical findings with Parasite Development in Trichinosis • Young adult migrating into mucosa of small intestine (24 – 72 hours) Nausea; Vomiting; Diarrhea; Abdominal pain. • Larvae in bloodstream and invading muscles (10 – 21 days) Periorbital edema; Conjunctivitis; Fever and chills; Muscle pain; Headache; Eosinophilia; Skin rashes; Painful breathing; Elevated muscle enzymes. • Larvae in Myocardium (14 – 21 days) Tachycardia; Edema of legs; Hypotensia; ECG changes; Elevated muscle enzymes. • Larvae in brain and meninges ( 14 – 28 days) Headache; Delirium; apathy, or altered conciousness; Stiff neck.
Trichinella spiralis TRICHINELLIASIS CLINICALLY • Thus a rising eosinophilia associated with fever, edema of the face, myalgia, and gastrointestinal disturbances provides strong presumptive evidence of trichinosis. LABORATORY EXAMINATION • Based on the detection of the larval worms in the muscle by biopsy and serologic and intracutaneous test.
Trichinella spiralis MUSCLE BIOPSY • Biopsies of the tendinous portions of the deltoid, biceps or gastroenemius muscles offers a specific though late method of diagnosis and if positive, affords definite proof of infection. • A positif diagnosis cannot be made before two weeks, and is seldom obtained, particularly in light infections, before three weeks. • The excised muscle is observed microscopically after compression between two slides or a special compressor, sectioning or digestion in an artificial gastric juice in order to concentrate the larvae.
Trichinella spiralis SEROLOGIC AND INTRACUTANEOUS TEST • Especially useful in diagnosis and in surveys, they include • Precipitation • Circumlarval microprecipitation • Complement fixation • Flocculation • Agglutination • Hemagglutination • Fluorescent antibody • Intracutaneous • Most workers consider that these tests are of greater diagnostic value than the detection of larval worms and that they have a relatively high degree of sensitivity.
Trichinella spiralis TRICHINELLIASIS DIFFERENTIAL DIAGNOSIS Trichinosis resembles many conditions : Due to the association with fever : Typhoid , Encephalitis , Myositis and Tetanus Association with a high eosinophilia : the tissue stages of Schistosomiasis ( Katayama syndrome ), Hook worm infection , Strongyloidiasis and other helmintic infections. Trichinosis may also resemble with collagen disorders such as : Periarteritis nodosa and Acute Rheumatoid arthritis.
Trichinella spiralis TRICHINELLIASIS TREATMENT • Spesific Treatment and symtomatic treatment is very important. There is no specific chemotherapeutic treatment for trichinosis. • Medical treatment is largely palliative, symptomatic and supportive, designed to tide the patient over the critical period. • The administration of chemotherapeutic agents againts the adult or larval worms has not been successful. • Benzimidazol most effective for Trichinella larvae before become cyst stage. • Albendazol is the drug of choice because absorbtion is good and free from side effect ; 400 mg twice a day for 8 to 14 days. • Mebendazole is allternative drug recommended 200mg – 400 mg • three times a day furthermore 400-500 mg three times a day for ten days . • In intestinal phase Corticosteroid is contra indication. In muscle invasion phase the patient with severe symptom must be take care in hospital and must be given corticosteroid high dose for 24-48 hours to be continuied with low dose for some weeks or months. In this phase the symptoms caused by inflamation and allergic reaction so corticosteroid is very important and anthelmintik is unnecessary.
Trichinella spiralis TRICHINELLIASIS PROGNOSIS • Although unfavorable in severe infections, is ordinarily good. • If survive the first 6 weeks of the acute illness, it will recover slowly and show no residual ill effects, although muscle pains may persist for 6 months. • Depend upon the location and number of larval trichinae, the age and physical condition of the patient, severity of symptoms, involvement of cardiorespiratory system, and complications. • In overwhelming infections death may take place in the second or third week, but more often it occurs in from 4 to 6 weeks.
Trichinella spiralis TRICHINELLIASIS PREVENTION • The ultimate eradication of trichinosis in man is dependent upon its elimination in hogs. • The prevalence can be greatly reduced by sterilizing garbage containing raw meat scraps, and by improving the sanitation of piggeries and slaughter houses. • The prevention of human trichinosis is dependent upon : • inspection of hogs in slaughter and packing houses, • the processing and refrigeration of pork products, * storage of pork in deep freeze units at - 37 *C * The cysts are destroyed by storage at -15*C for 20 days or more * pork must be cooked at temperature not lower than 58,3 *C Irradiation with cobalt-60 which kill the cysts. • the education of housewife with regard to the through cooking of pork.
Trichinella spiralis TRICHINELLIASIS EPIDEMIOLOGY • EPIDEMICS • Trichinosis has a cosmopolitan distribution but is rare or absent in India, Australia and some Pasific islands. • In recent years small and large epidemics have occurred, among these are : • Greenland in 1947 with 300 cases • Poland in 1951 and 1959 with 92 and 308 cases • Germany in 1951 with 436 cases • Liverpool, England in 1953 with 53 cases • Romania in 1955 with 24 cases. • There has been an increase in small outbreaks in the United States of America since 1930, the last being in Pennsylvania in 1961.