Download
1 / 49
490 likes | 694 Views
Use of “low dose” CT for routine urological investigation: renal colic and haematuria. Dr Chris O’Donnell Radiologist – MIA Victoria. Low dose CT. ACCC – Competition and Consumer Act 2010. misleading or deceptive conduct. Summary of presentation. “low dose” CT

E N D
Use of “low dose” CT for routine urological investigation:renal colic and haematuria Dr Chris O’Donnell Radiologist – MIA Victoria
ACCC – Competition and Consumer Act 2010 • misleading or deceptive conduct
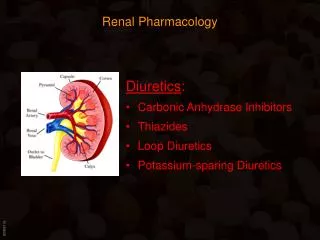
Summary of presentation • “low dose” CT • urological investigation using low dose CT • CT KUB and CT IVU/P • renal colic • haematuria
“Low dose” CT • CT scanner that has software/hardware improvements to reduce radiation dose or exposure whilst producing high quality diagnostic images
Ionizing radiation • “ionizing” • energy that can move an electron from its normal orbit • effect • breaks chemical bonds in DNA • rapidly dividing cells cannot repair the DNA
Dose • measure of the energy deposited by ionizing radiation per unit mass • measured as joules per kilogram • represented by the SI unit, Gray (Gy) • dose equivalent • biological effect of the ionizing radiation/energy deposition • represented by the SI unit, Sievert (Sv) • Sv = Gy x WF (1:1) • we talk about Sv in looking at clinical radiation risk
Relative doses (conventional CT) • background radiation = 3mSv/year • air travel • 10 hr. flight = 0.06mSv, via the poles = 0.1mSv • CXR = 0.1mSv (1/30 of background) • AXR = 0.7mSv (1/4) • CT brain = 2mSv (2/3) • CT abdo/pelvis = 6.8 – 35, mean 14mSv (~5x) • nuclear renal scan = 3.3mSv (1x) • coronary angiogram (diagnostic) = 7mSv (~2x) • interventional cardiac = 14mSv (~5x) • CT coronary angiogram = 16mSv (>5x)
Biological effects of ionizing radiation • stochastic effects * • occur by chance • cancer and genetic effects • usu. occurs years after exposure • as dose increases, probability of effect increases • not certain even if very high doses • no threshold • non-stochastic effects • threshold dose below which they do not occur • exposure = effect • magnitude of the effect is directly proportional to the size of the dose • typically very large dosages of radiation received in a short amount of time • effects will often be evident within hours or days • erythaema, skin and tissue burns • cataract formation • sterility • bone marrow, GI tract, CNS suppression • radiation sickness and death
principle of ALARA • As Low As Reasonably Achievable (dose) • cannot dose reduce to 0 • “background” radiation • do have to manage patients • practicalities • fewer X-ray procedures or alternatives e.g. MRI • reduces total dose • prolonged intervals between exposure • allowing DNA to repair • not children/pregnancy • more dividing cells • lifetime “cumulative” risk
How do I do this (ALARA)? • personal supervision of the CT examination (by a radiologist) • restrict the regions of scanning • suggest different scanning procedures where appropriate • US for CT (children/young women) • MRI for CT (MRI is often better for many conditions/body parts)
US • no ionizing radiation • common usage • funded by Medicare • value in urology • bladder and prostate • solid v cystic renal masses • screening of the urinary tract • children • often not definitive
MRI • no ionizing radiation • excellent alternative for many conditions • limited by access, Medicare funding • from 1/11/12 improved access esp. for children • from 1/11/13 – adults ??? • CT still best for • acute trauma • acute chest/abdominal pathology including renal colic • oncology staging • CT angiography • ? general urology
CT • amazing technology
“Low dose” CT • number of strategies by manufacturers to reduce the exposure • improved efficiency of x-ray detectors • improved analysis of the data • Adaptive Statistical Iterative Reconstruction (ASIR)
ASIR • improved mathematical reconstruction of the image data • only possible now that we have very fast PCs • “retrofit” to currently installed CT scanners • upgrade in the hardware and software of image reconstruction • typically >50% reduction in radiation dose • no compromise in image quality
ASIR –noisy images made better conventional reconstruction ASIR reconstruction
MIA committed to retrofit all CT scanners to “low dose” 70% completed Moorabbin Radiology
CT images – reduce dose conventional CT “ low dose” CT
What does this mean? • less reluctance to perform CT • urology • we can recommend CT as the investigation of choice for many suspected renal pathologies especially in renal colic and haematuria
IVU/P • intravenous urogram or pyelogram • traditional radiographic study of renal tract • intra-venous injection of iodine-based radiographic contrast • excretion via the kidney into the collecting systems • now not available – technical reasons • CT equivalent – CT IVU/P
What is a CT IVU/P? • 3 components/phases • 1. “non-contrast” through renal tract for stones (CT KUB) • 2. “parenchymal or nephrogram” contrast phase through whole abdomen for viscera • 3. delayed “excretory” contrast phase through renal tract for collecting system • phases 2 and 3 can be combined for younger patients (to reduce radiation dose) • i.e. give an initial injection of contrast, wait 20 mins than do parenchymal phase with a second contrast injection
CTIVU/P non-contrast mixed parenchymal and excretory phases
Renal colic • all stones are radio-opaque on CT • 90% on plain radiographs (not uric acid) • look for stone in the ureter with signs of ureteric obstruction • swollen kidney • thickening of perinephric fat • dilatation of the ureter above the stone and collapse beyond • 3 sites i.e. PUJ, VUJ and pelvic brim
CT KUB for renal colic • CT kidney, ureter, bladder • only the preliminary portion of the CT IVU/P • does not need contrast injection • urologists often like an addition radiograph to follow the stone passage • preliminary “scout” film Low-Dose Versus Standard-Dose CT Protocol in Patients with Clinically Suspected Renal Colic AJR 2007 188 (4) 927-933
CT KUB for stone/calculus swollen kidney stone at VUJ
Haematuria • origin • kidney, ureter, bladder, urethra • tumour (RCC, TCC), infection, stone, bleeding diathesis • CT IVP is a very good overall study • kidney, ureter, bladder (not urethra) • tumour (RCC, TCC), stone • c/w ultrasound – especially children, younger women c/o radiation dose
Examples RCC TCC ureter TCC bladder
Beware • a –ve CT IVU/P does not fully exclude TCC of the bladder • requires • urine cytology • cystoscopy
Conclusion (1) • CT is still a very useful imaging modality • funded by Medicare • investigation of choice in many conditions and body parts • radiation dose is an issue • multiple scans, children and young women • low dose CT is an important advance • MIA Victoria is committed to this strategy • retrofit all CT scanners to ASIR
Conclusion • radiation dose is now less of an issue c/o new “low dose” CT technology • e.g. urology • CT KUB for colic or CT IVU/P for haematuria • very comprehensive examinations • recommended