Download
1 / 69
710 likes | 989 Views
INTRACRANIAL PRESSURE : Hydrocephalus, Meningitis, Head Injury, Brain Tumors Fall 2009. WHY DOES IT HAPPEN?. Brain tissue + blood + CSF = skull volume. MONROE-KELLIE HYPOTHESIS. Because of the limited space for expansion within the skull

E N D
INTRACRANIAL PRESSURE:Hydrocephalus, Meningitis, Head Injury, Brain Tumors Fall 2009
WHY DOES IT HAPPEN? • Brain tissue + blood + CSF = skull volume
MONROE-KELLIE HYPOTHESIS • Because of the limited space for expansion within the skull • An in any one of the components a change in the volume of the other
COMPENSATION • Shifting of CSF • INCREASED absorption of CSF • DECREASED cerebral blood volume
WITHOUT COMPENSATION • ICP will rise • DECREASED cerebral perfusion stimulates edema shifts brain tissue Through openings in the rigid dura HERNIATION DEATH
DECREASED CEREBRAL BLOOD FLOW • ICP REDUCES CEREBRAL BLOOD FLOW ISCHEMIA CELL DEATH • SYSTEMIC RESPONSE: Vasomotor centers stimulated BP accompanied by slow bounding pulse and respiratory irregularities
EFFECTS OF CO2 ON CEREBRAL BLOOD FLOW • CO2 partial pressure cerebral vasodilation leads to INCREASED cerebral blood flow and ICP • CO2 partial pressure cerebral vasoconstriction
BODY’S COMPENSATION FOR CEREBRAL EDEMA • GOAL: MAINTAIN BLOOD FLOW AND PREVENT TISSUE DAMAGE • Autoregulation: brain changes the diameter of its blood vessels automatically to maintain a constant cerebral blood flow during alterations in systemic blood pressure • Decreasing production and flow of CSF
CUSHING’S RESPONSE • Seen when cerebral blood flow decreases significantly • With ischemia vasomotor centers increases arterial pressure to overcome the ICP • Sympathetic response causes a rise in systolic BP, widening pulse pressure and reflex slowing of the heart rate • MUST HAVE IMMEDIATE INTERVENTION • CAN RECOVER AT THIS POINT IF TREATED RAPIDLY
CUSHING’S TRIAD • At a certain volume and pressure the brains ability to autoregulate becomes ineffective leading to ischemia and infarction • See in patient: mental status changes and bradycardia, hypertension and bradypnea • IF NO INTERVENTION leads to HERNIATION OF THE BRAIN STEM
HERNIATION OF THE BRAIN STEM • Shifting of brain tissue • Area that is shifted has pressure on it • Resulting in decreased blood supply • Resulting in cerebral ischemia • Resulting in INFARCTION and BRAIN DEATH
PATHOLOGIC CONDITIONS THAT CAUSE IIP • Head injury, CVA • Brain tumor • Intracranial surgery • Meningitis • Encephalitis • Subarchnoid hemorrhage
EARLY SYMPTOMS OF IIP • ***change in LOC: Slowing of speech Delay in response to verbal suggestions Irritability, Restlessness, resp effort • Changes in pupils • Weakness in one extremity/ 1 side of body • Headache constant increasing in intensity
LATE SYMPTOMS OF IIP • Deterioration of LOC leading to coma • Sluggish, unequal response of pupils to light • HR ; RR ; bradycardia to tachycardia • BP and temperature rise • Pulse pressure widens • irregular respiratory pattern: Cheyne Stokes • Projectile vomiting • Hemiplegia, decorticate/decerebrate posturing, bilateral flaccidity before death • Loss of brain stem reflexes
Neurologic Nursing Assessments • LOC • Pupil response • VS • Motor activity
ASSESSMENT OF LEVEL OF CONSCIOUSNESS Indication of the highest level of cerebral activity EVALUATION IS DONE BY: • Determining degree of alertness • Orientation to person, place, time • Ability to awaken • Degree of lethargy • Status of reflexes (gag, swallow, etc)
ASSESSMENT OF PUPILS • Determines reaction to light • NORMAL: the pupils constrict rapidly and equally to light (PERLA) • ABNORMAL: unequal reaction, abnormal position of pupils
ASSESSMENT OF VS INDICATING IIP • Pulse decreases • Respiration decreases • BP increases • Temperature increases
ASSESSMENT OF MOTOR ACTIVITY • Watch hand and feet movement • Have pt squeeze your fingers • Look for change in facial muscles • Look for inequality of motor strength, generalized weakness, tremors, ataxia
ASSESSEMENT OF TEMPERATURE • Increased temperature indicates increased intracranial pressure • CAUSE: irritation or damage to temperature regulating mechanism in brainstem
SEIZURE PRECAUTIONS • Pad side rails • Have oxygen and suction available • Observe for seizures
ASSESSMENT/DIAGNOSTICS • CT scan • MRI • PET (positive emission tomography)
MANAGEMENT • GOAL IS TO RELIEVE INCREASED ICP HOW? • cerebral edema • volume of CSF • cerebral blood volume while maintaining cerebral perfusion
MONITOR ICP • Intraventricular catheter (ventriculostomy) • Subarachnoid bolt • Epidural/subdural catheter • Fiberoptic transducer-tipped catheter placed in subdural space or the ventricle
GOALS: decreasing cerebral edema • Administer osmotic diuretics mannitol(Osmitrol) • Administer coricosteroids dexamethasone (Solumedrol, Medrol) • Restrict fluids • Drain CSF
GOAL: maintaining cerebral perfusion • GOAL: Improve cardiac output • HOW: Using fluid volume and inotropic agents (dobutamine hydrochloride) • EFFECTIVENESS OF CARDIAC OUTPUT OUTCOME ASSESSED INDICATING SUCCESS AT : cerebral perfusion pressure maintained at greater than 70 mm Hg
GOAL: Reducing CSF and intracranial blood volume • Use of drains to remove CSF • This reduces ICP and restores cerbral perfusion pressure • CAUTION: overdrainage causes collapse of the ventricles
GOAL: controlling fever • Fever increases cerebral metabolism and increases cerebral edema • Antipyretics • Cooling blankets
GOAL: maintaining oxygenation • Maintain oxygenation • Monitor arterial blood gases
GOAL: Reducing metabolic demands • Reduce cellular metabolic demands • Administer barbiturates: nembutal, pentothal, diprivan • Administer opiods (morphine sulfate or fentanyl citrate) with ventilated clients to decrease agitation • Administer paralyzing agents vercuronium bromide or cisatracurium (Nimbex): agitation. Must be used with sedation/analgesia
ASSESSMENTS NOTED WITH ICP BASED ON LOCATION IN BRAIN • ICP on frontal lobes leads to Cheyne Stokes respirations • ICP in the midbrain causes hyperventilation • ICP in the lower portion of the brain stem (pons and medulla) leads to irregular respirations and eventually apnea
HYDROCEPHALUS • Condition present at birth or resulting from other cause in which there is an abnormal amount of CSF volume in the intracranial cavity. • The fluid accumulates in the ventricles of the brain
TYPES OF HYDROCEPHALUS INTERNAL NON-COMMUNICATING: • Blockage within the ventricles keeping the CSF from going to the subarachnoid space CAUSES: • developmental malformations • Neoplasms • Infections • trauma
TYPES OF HYDROCEPHALUS CONTINUED INTERNAL COMMUNICATING HYDROCEPHALUS: • Occurs when the obstruction is in the subarachnoid cistern at the base of the brain or in the subarachnoid space. • There is no blockage in the ventricles • Fluid pathways are open • Fluid is not absorbed into the spinal subarachnoid space
S & S OF HYDROCEPHALUS EARLY • Increased head circumference • Bulging fontanels • Cranial sutures separate • Signs of increased ICP
S & S OF HYDROCEPHALUS • LATE: • Macewen’s sign (cracked pot) • Setting sun sign (bulging eyes, schlera visible above iris) • Opisthtonus (arched back) • Frontal bossing (forehead enlargement)
TREATMENT OF HYDROCEPHALUS • Correction of cause of obstruction • Ventricular shunting procedures
SHUNTS • Ventricular catheter with a oneway flow valve and a distal catheter • Designed to open at a predetermined pressure and close when the pressure falls below that level • Allows the CSF to go into the general circulation
Types of shunts • Ventriculoperitoneal (VP) – one of choice • OLDER FORMS: • Ventriculpleural • ventriculoatrial
PROBLEMS WITH SHUNTS • Infections • Tubing becomes kinked, plugged or separates • Needs to be replaced when grows
POSTOP NURSING CARE • Position on unoperated side to prevent pressure on the shunt valve • Keep flat to prevent too rapid reduction of intracranial fluid (when the ventricular size is reduced too fast the cerebral cortex pulls away from the dura and produces a subdural hematoma)
COMPLICATIONS • SHUNT INFECTION: look for inflammation at the operative site and along the shunt tract and increased intracranial pressure symptoms • TREATMENT: intraventricular and IV antibiotics • SHUNT OBSTRUCTIONS: look for S & S of increased intracranial pressure • TREATMENT: return to surgery
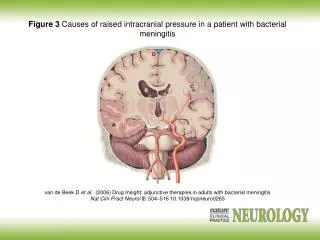
Other causes of IICP: MENINGITIS DEFINED: Infection of pia mater, arachnoid membrane and CSF filled subarachnoid space due to bacteria, virus, or fungal organism
S & S OF MENINGITIS • NEONATE: hypothermia or fever depending upon maturity, refuse to eat, poor muscle tone • INFANTS: fever and high pitched cry, headache, bulging fontanel • CHILDREN/ADOLESCENTS: fever, photophobia, headache, nuchal rigidity, positive Kernigs and Brudzinski’s signs
SIGNS AND SYMPTOMS COMMON TO ALL AGES • Irritability • Seizures • vomiting
DIAGNOSIS OF MENIGITIS LP: CSF examined Pressure measured • Normal: 0 to 15 mm Hg • Increased ICP: greater than 15 mm Hg CSF sent to lab to identify organism • Gram stain (preliminary identification • Blood Cell Count: increased WBC • Glucose: decrease in glucose • Protein: increase in protein
TREATMENT OF MENINGITIS • Antibiotics after LP and sending of CSF • Penicillin (ampicillin, piperacillin) • Cephalosporins (cetriaxone sodium, defotasime sodium) • Vancomycin hydrochloride alone or with Rifampin • Dexamethasone given 15-20 min befoe first dose of antibiotic and every 6 hours for next 4 days