Download
1 / 1
10 likes | 148 Views
Opportunistic Intervention for Smoking Cessation Among Hospitalized Smoker Patients in TTSH. P. A. S. A. S. P. D. P. D. D. A. S. No counselor. S. A. D. P. P. D. S. A. MISSION STATEMENT. PARETO CHART. TEAM MEMBERS. INTERVENTION. # 5. # 4. # 3.

E N D
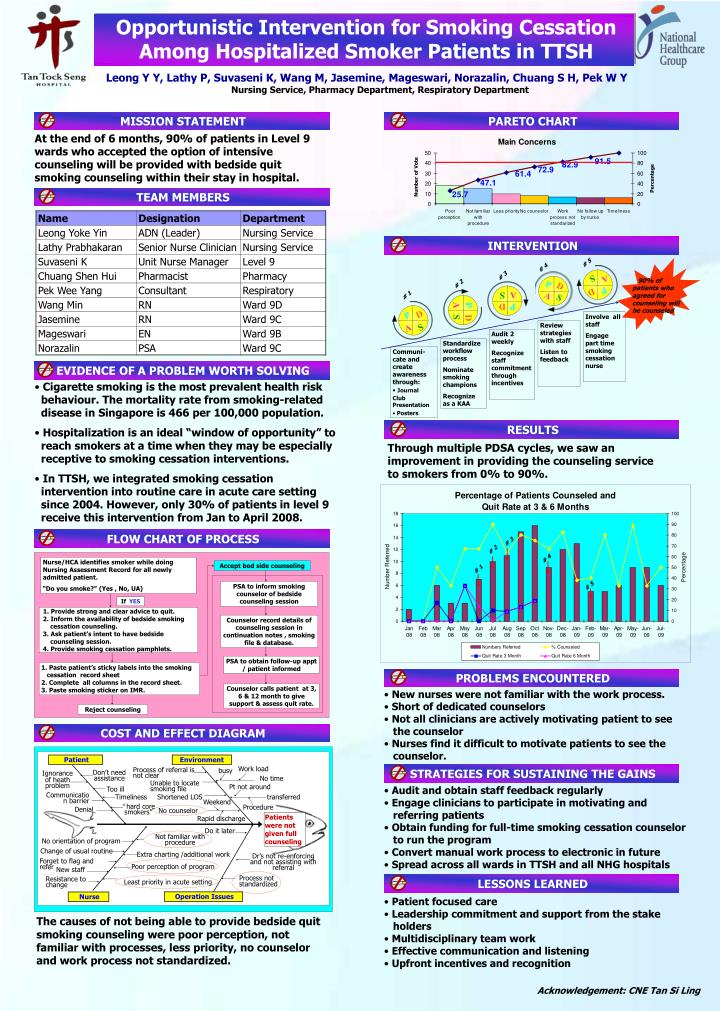
Opportunistic Intervention for Smoking Cessation Among Hospitalized Smoker Patients in TTSH P A S A S P D P D D A S No counselor S A D P P D S A MISSION STATEMENT PARETO CHART TEAM MEMBERS INTERVENTION # 5 # 4 # 3 90% of patients who agreed for counseling will be counseled # 2 # 1 EVIDENCE OF A PROBLEM WORTH SOLVING RESULTS FLOW CHART OF PROCESS Nurse/HCA identifies smoker while doing Nursing Assessment Record for all newly admitted patient. “Do you smoke?” (Yes , No, UA) Accept bed side counseling PSA to inform smoking counselor of bedside counseling session If YES 1. Provide strong and clear advice to quit. 2. Inform the availability of bedside smoking cessation counseling. 3. Ask patient’s intent to have bedside counseling session. 4. Provide smoking cessation pamphlets. Counselor record details of counseling session in continuation notes , smoking file & database. PROBLEMS ENCOUNTERED PSA to obtain follow-up appt / patient informed • Paste patient’s sticky labels into the smoking • cessation record sheet • 2. Complete all columns in the record sheet. • 3. Paste smoking sticker on IMR. Counselor calls patient at 3, 6 & 12 month to give support & assess quit rate. COST AND EFFECT DIAGRAM Reject counseling STRATEGIES FOR SUSTAINING THE GAINS Unable to locate smoking file Procedure Rapid discharge Patient Environment Work load busy Process of referral is not clear Don’t need assistance Ignorance of heath problem No time Pt not around Too ill Timeliness Shortened LOS transferred Communication barrier Weekend LESSONS LEARNED “hard core smokers” Denial Patients were not given full counseling Do it later Not familiar with procedure No orientation of program Change of usual routine Extra charting /additional work Dr’s not re-enforcing and not assisting with referral Forget to flag and refer Poor perception of program New staff Process not standardized Resistance to change Least priority in acute setting Operation Issues Nurse Leong Y Y, Lathy P, Suvaseni K, Wang M, Jasemine, Mageswari, Norazalin, Chuang S H, Pek W Y Nursing Service, Pharmacy Department, Respiratory Department At the end of 6 months, 90% of patients in Level 9 wards who accepted the option of intensive counseling will be provided with bedside quit smoking counseling within their stay in hospital. Involve all staff Engage part time smoking cessation nurse Review strategies with staff Listen to feedback Audit 2 weekly Recognize staff commitment through incentives Standardize workflow process Nominate smoking champions Recognize as a KAA • Communi-cate and create awareness through: • Journal • Club Presentation • Posters • Cigarette smoking is the most prevalent health risk • behaviour. The mortality rate from smoking-related • disease in Singapore is 466 per 100,000 population. • Hospitalization is an ideal “window of opportunity” to • reach smokers at a time when they may be especially • receptive to smoking cessation interventions. • In TTSH, we integrated smoking cessation • intervention into routine care in acute care setting • since 2004. However, only 30% of patients in level 9 • receive this intervention from Jan to April 2008. Through multiple PDSA cycles, we saw an improvement in providing the counseling service to smokers from 0% to 90%. # 3 # 2 # 4 # 1 # 5 • New nurses were not familiar with the work process. • Short of dedicated counselors • Not all clinicians are actively motivating patient to see • the counselor • Nurses find it difficult to motivate patients to see the • counselor. • Audit and obtain staff feedback regularly • Engage clinicians to participate in motivating and • referring patients • Obtain funding for full-time smoking cessation counselor • to run the program • Convert manual work process to electronic in future • Spread across all wards in TTSH and all NHG hospitals • Patient focused care • Leadership commitment and support from the stake • holders • Multidisciplinary team work • Effective communication and listening • Upfront incentives and recognition The causes of not being able to provide bedside quit smoking counseling were poor perception, not familiar with processes, less priority, no counselor and work process not standardized. Acknowledgement: CNE Tan Si Ling