Methods
Cognitive and Psychiatric Status in Pediatric Multiple Sclerosis Weisbrot, D. ¹, Charvet , L. ² , Serafin , D. ² , Belman , A. ² , Milazzo, M. ² , Preston, T. ² , Seibert, M. ² , Moadel , T. ² , Krupp LB.² , ³ Lourie Center for Pediatric MS

Methods
E N D
Presentation Transcript
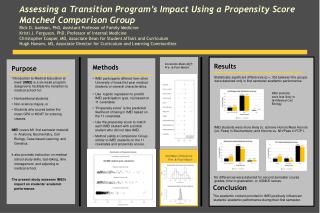
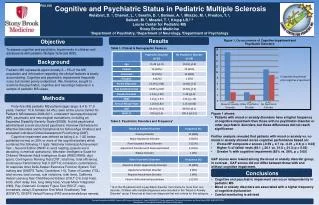
Cognitive and Psychiatric Status in Pediatric Multiple SclerosisWeisbrot, D. ¹, Charvet, L.², Serafin, D. ², Belman, A. ², Milazzo, M. ², Preston, T.², Seibert, M. ², Moadel, T. ², Krupp LB.²,³ Lourie Center for Pediatric MS Stony Brook Medicine¹Department of Psychiatry, ²Department of Neurology, ³Department of Psychology P04.106 Results Objective Figure 1. Co-occurrence of Cognitive Impairment and Psychiatric Disorders Table 1. Clinical & Demographic Features To assess cognitive and psychiatric impairments in children and adolescents with pediatric Multiple Sclerosis (MS). Background Pediatric MS represents approximately 3 – 5% of the MS population and information regarding the clinical features is slowly accumulating. Cognitive and psychiatric impairments frequently occur but remain poorly understood. We, therefore, sought to examine the psychiatric, cognitive and neurologic features in a sample of pediatric MS cases. Methods n=20 n=5 n=20 Forty-five (45) pediatric MS patients (age range: 8.4 to 17.9 years, median: 15.6, female: 64.4%), seen at the Lourie Center for Pediatric MS between 2006-2011, underwent neuropsychological (NP), psychiatric and neurologicalevaluations, including an Expanded Disability Severity Scale (EDSS). A child psychiatrist administered a semi-structured psychiatric interview (Schedule for Affective Disorders and Schizophrenia for School-Age Children)and evaluated individual Global Assessment Functioning (GAF). Cognitive impairment was defined as failing (i.e. 1 SD below published norms) on 20% or more of the cognitive battery which contained the following 11 tests: Wechsler Individual Achievement Test – Second Edition (WIAT-II; word reading, pseudo word decoding, numerical operations), Wechsler Intelligence Scale for Children/ Wechsler Adult Intelligence Scale (WISC/WAIS; digit span), Contingency Naming Test (CNT; total time, total efficiency), Continuous Performance Test II (CPT-II; omissions, commissions, hit response time) Delis-Kaplan Executive Function System Trail making test (DKEFS Trails; Conditions 1-5), Tower of London (TOL; total moves, total correct, rule violations, total time), California Verbal Learning Test-Child/Second Edition (CVLT-C/II; total trials, list B, short delay free, long delay free), Visual-Motor Integration (VMI), Rey-Osterrieth Complex Figure Test (ROCF; copy, immediate, delay), Expressive One Word Vocabulary Test (EOWVT), DKEFS Verbal Fluency (FAS and animals/boys names). • Figure 1 shows: • Patients with mood or anxiety disorders have a higher frequency of cognitive impairment than those with no psychiatric disorderor other psychiatric disorders, but these differences did notreach significance. • Further analysis revealed that patients with mood or anxiety vs. no mood or anxiety showed worse cognitive performance based on: • Worse NP composite z scores (-0.59 + 0.7 vs. -0.01 +0.6; p = 0.02) • Higher % of failed tests (49.1 + 26.1 vs. 31.8 + 21.3; p = 0.02) • Greater % with cognitive impairment (85% vs. 56%, p = 0.05) • GAF scores were lowest among the mood oranxiety disorder group, in contrast , GAF scores did not differ between those with and without cognitive impairment. Table 2. Psychiatric Disorders and Frequency* Conclusions . • Cognitive and psychiatric impairment can occur independently in pediatric MS • Mood or anxiety disorders are associated with a higher frequency of cognitive dysfunction • Careful monitoring is advised *16 of the 25 patients with a psychiatric disorder met criteria for more than one disorder. Children with multiple diagnoses were included in the “Mood or Anxiety Disorder” group if they had at least one diagnosis that met criteria for this category. Research funded by the NMSS “Pediatric MS Centers of Excellence” Award, NMSS #PP1017 and supported by The Lourie Foundation and Stony Brook GCRC (#5MO1RR10710). Stony Brook is 1 of 6 regional Pediatric MS Centers of Excellence