Download
1 / 79
790 likes | 1.04k Views
Ambulatory Electronic Health Records 2010. Sizzle or Fizzle? Bob Hoyt MD FACP February 5 2010. Learning Objectives After presentation participants should be able to: . Enumerate why the federal government is interested in EHRs

E N D
Ambulatory Electronic Health Records 2010 Sizzle or Fizzle? Bob Hoyt MD FACP February 5 2010
Learning ObjectivesAfter presentation participants should be able to: • Enumerate why the federal government is interested in EHRs • Compare and contrast the benefits and obstacles related to ambulatory EHRs • List Medicare and Medicaid eligibility criteria and reimbursement plans • Discuss the meaning of meaningful use • Provide examples of commonly purchased EHRs
Disclaimers • I have no conflicts of interest to report • I will be discussing outpatient and not inpatient electronic health records • My comments will be general and might not apply to every medical office scenario
Ad in Wall Street Journal 2/3/2010Is this a new market strategy?
EHRs will not solve everything“Technology is not the destination, it is the transportation” Dr. Safron AMIA
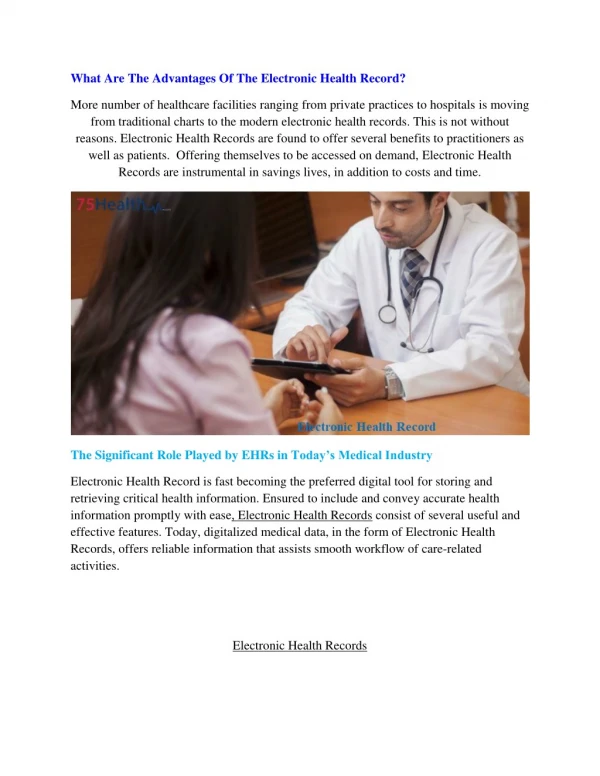
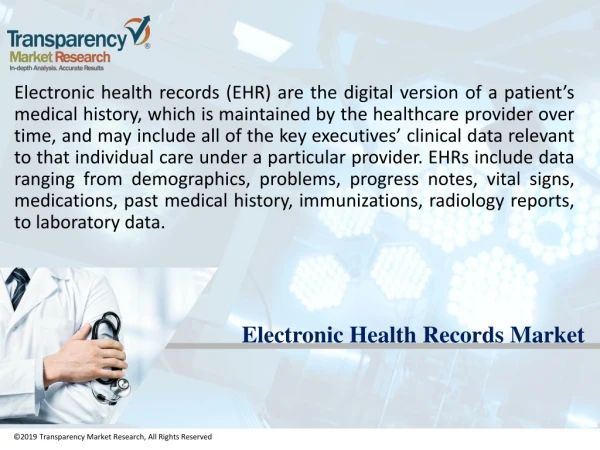
Why is the government promoting EHRs? • EHR adoption rates are low • According to the Institute of Medicine (IOM): • Paper charts are inadequate for modern medicine • EHRs will: improve the quality of medical care, improve patient safety, decrease inefficiencies/costs and produce aggregated data for mining
What is the government strategy? • In 2004 Executive Order 13335 mandated interoperable EHRs for every Americanby 2014 and created the Office of the National Coordinator for Health Information Technology (ONC) • To do this there was a need to also promote Health Information Organizations (HIOs) and the Nationwide Health Information Network (NHIN) • 2009 ARRA supports EHRs, HIOs and the NHIN
Ambulatory EHR Adoption Rate NEJM July 3 2008
NEJM Article Conclusions • Sample of 2758 physicians from the AMA physician register (62% response rate) • Survey excluded residents in training, osteopaths and federal physicians • Overall, 13% of physicians surveyed had some type of EHR but only 4% had a comprehensive type of EHR (CPOE and CDSS) • Satisfaction level was reasonably good
Ambulatory EHR Adoption 100 25 80 20 60 15 40 10 5 20 0 0 Level of EHR Function Size of Practice > 50 physicians Basic System 13% 50% Percentage Percentage Fully Functional 1 - 3physicians 4% 9% DesRoches, N Engl J Med, 2008 12
National Ambulatory Medical Care Surveys (NAMCS) 2001-2009 Non-federal physician mail survey
Paper charts are inadequate • Often illegible • Non-structured data so can’t be mined or shared easily • Difficult to generate reports of any kind • Record rooms and chart pulls are costly • Difficult to retrieve past notes, labs, x-rays, etc • Paper charts missing 25% of the time. When chart is available labs, etc are missing 14% of the time • Can’t be accessed from home/hospital or shared by multiple users simultaneously • Can’t provide clinical decision support
Do EHRs improve the quality of medical care? • Although there are a few studies that suggest physicians are more likely to follow outpatient (clinical practice guidelines) and inpatient (order sets) embedded EHR recommendations, there are an equal number of studies that suggest no impact on physician behavior or patient outcomes
Do EHRs improve patient safety? • Most studies have evaluated EHR generated drug-related alerts and reminders for preventive care • Most studies come from the same 4 medical centers • “Alert fatigue” a huge problem with e-prescribing • Reminders are ignored because there is not enough time to act on every preventive medicine measure • Bottom line: we have little evidence to suggest improved patient safety due to EHRs • Also, there is concern that any new technology may actually cause safety issues (“e-iatrogenesis”)
Do EHRs save money? • Yes, potentially through these mechanisms: • Decreased record room requirements and chart pull costs leading to decreased FTEs • Improved coding • Decreased fax and mail costs • Decreased transcription costs with use of templates and voice recognition • EHR generated “pay for performance” reports • Fewer “call backs” from pharmacists with e-prescribing
Example of financial benefits Miller et al. Health Affairs 2005;24:1127-1137
Benefits of aggregated data • Relationship of Primary Care Physicians’ Patient Caseload with Measurement of Cost Performance Nyweide DJ et al. JAMA 2009;302 (22):2444-2450 Conclusion: “relatively few primary care physician practices are large enough to reliably measure 10% relative differences in common measures of quality and cost performance among fee-for-service Medicare patients” • Large organizations like the VA and Kaiser-Permanente can show the benefits of aggregated structured data
Subgroup Differences in Triglyceride by High Density Level Cholesterol Ratios Over Age
EHR Obstacles • Cost (in the face of possible 21% Medicare cuts!) • Physician Resistance http://www.youtube.com/watch?v=Pk7yqlTMvp8 • Workflow changes • Legitimate privacy and security concerns • Possible need for in-house IT support • Initial loss of productivity • Integration with other systems: practice management, lab, PACS, HIEs, etc. • Lack of interoperability standards • Lack of high quality studies showing unequivocal patient benefit and clear cut ROI
How Much Do Typical EHRs Cost ?Health Affairs Sept/Oct 2005 Miller et al Health Affairs 2005;24:1127-1137
Some conclusions from this study • Wide cost differences in software often due to negotiating differences • Practices stopped using transcription • Average time for ROI was 2.5 years but one practice was projected to take 9 years and two others “never” • 3 practices had serious billing issues • Clinicians worked longer hours for average of 4 months
Diffusion of Innovation:Expect 50% to be slow adopters of any innovation Diffusion of Innovation, Everett Rogers 1995
Two recent negative studies • November 2009: A. Jha (in press) looked at quality measures (example heart failure tx) and length of stay (LOS) in 3000 hospitals and tried to tie that to hospitals that had an advanced EHR, basic EHR or no EHR. Bottom line: No significant differences • January 2010: D. Himmelstein looked at hospital computerization, costs and quality of care at 4000 hospitals 2003-2007. Bottom line: marginal improvement in process measures of quality but no reduction in administrative or overall costs
Health Information Technology for Economic and Clinical Health Act (HITECH) • Part of the American Recovery and Reinvestment Act (ARRA) of 2009 • $14-27 billion to support the adoption of electronic health records for all Americans in the next decade • Multiple other ARRA programs support HIT
Federal HIT programs and grants • Medicare/Medicaid EHR reimbursement program • HIT extension program (70 centers) • Curriculum development centers • Community college consortia for HIT education • Program of assistance for university-based training • Competency exam for individuals completing non-degree training • Strategic health advanced research projects (SHARP) • Beacon community cooperative agreement program • State HIE cooperative agreement program
Transformational Change in Health Care Delivery & Population Health The government sees Health IT as critical forhealthcare transformation Technology Adoption 2012? TIME 2004
Evolution of the EHR Record on stone or paper No Record Electronic Record Interoperable Electronic Record Verbal Record
Three important levels of HIT National Office EHR Local, state or regional HIOs N H I N HIO 1 HIO 2 Patient Portal PHR Hospitals Payers
EHR reimbursement by CMS • Physicians must be eligible for reimbursement by Medicare or Medicaid criteria • EHRs must be certified by an organization such as the Certification Commission for Health Information Technology (CCHIT) • Physicians must demonstrate “meaningful use” which we will define in future slides
Federal Meaningful Use Notices • CMS issued a notice of proposed rulemaking (NPRM) on Jan 13 2010 on “Meaningful Use” with an unclear date when it would be effective • ONC issued a interim final rule (IFR) on EHR certification criteria related to meaningful use on Jan 13 2010; effective Feb 12 2010 • Comments on both are due Mar 15 2010 • ONC will issue a NPRM relating to the testing and certification of complete EHRs and EHR Modules sometime in 2010
Meaningful use • MU Categories • Improving quality, safety, efficiency and disparities • Engage patients/families in their healthcare • Improve care coordination • Improve public and population health • Ensure adequate privacy and security protection • There will be three stages of meaningful use with stage 1 beginning in 2011
How will meaningful use be accepted? • The public will have 60 days to make comments, so expect changes • Already, many organizations have voiced concerns, primarily about new reporting requirements that will likely have glitches and cost physicians time and money • Will CMS be ready to receive reports? • Will payments to physicians be timely or slowed down by bureaucracy? • Will the cost to purchase an EHR increase as a result of matching meaningful use criteria?
Vendors who offer guarantee their EHR will match all criteria • PracticeFusion, Allscripts, Ingenix, Athenahealth, ChartLogic, E-MDs, GE Healthcare, Medsphere, NextGen, Noteworthy Medical systems, eClinicalWorks and SourceMedical
EHRs certified for 2011 but will have to be retested to match MU criteria
Medicare Reimbursement • Payments = 75% of Medicare allowable charges (Part B claims; Part C for Medicare Advantage) for the year, subject to max payments of $18K, $12K, $8K, $4K and $2K for years 1-5 • “Physicians” = MD, DO, Dentists, Oral surgeons, Podiatrists, Optometrists and Chiropractors • 10% extra incentive if practice is in under-served area • $0 if first year adoption is after 2014 • Does not apply to hospital based physicians • Includes Medicare Advantage programs and hospitals • First year reporting period is 90 continuous days
Medicaid reimbursement • “Unlike the Medicare incentive programs, the Medicaid program allows eligible providers to receive an incentive payment even before they have begun to meaningfully use certified EHR technology” • “Medicaid clinicians would have to attest to having adopted, (that is, acquired and installed) or commenced utilization of (that is, implemented) certified EHR technology; or expanded (that is, upgraded) the available functionality of certified EHR technology and commenced utilization at their practice site” • States will receive 90% reimbursement from the federal government for administrative costs to administer the EHR program as well as the money to reimbursement physicians
Other information and resources to help make the decision to buy now, wait or not buy
More than 250 EHRs available! Expensive (Enterprise) Moderately Expensive Less expensive “Free” Open Source Practice Fusion SynaMed MDBug Amazing Charts Praxis Soapware eClinicalWorks E-MD Allscripts Misys Etc Epic Vista AHLTA Cerner McKesson
Free EHR Search Engine www.ehrscope.com Results after applying 13 filters = 16 matches
KLAS research firm • Firm rates EHRs and practice management systems each year • Ratings come largely from customers: EHR performance, vendor reliability, support, etc • Ratings are based on practice size • There is a charge for their services but physicians who are willing to complete a questionnaire on current IT use can evaluate individual vendors free of charge
KLAS results for 2009 • Greenway Medical PrimeSuite was #1 for four years in a row for practices 6-25 physicians; #1 for two years in a row for practices of 2-5 physicians • Epic Systems was #1 for practices >100 physicians • eClinicalWorks was #1 for practices 26-100 physicians