Download
1 / 81
930 likes | 2.04k Views
Gestational Trophoblastic Disease (GTD). Types of GTD. Benign Hydatidiform mole/molar pregnancy (complete or incomplete) malignant Invasive mole Choriocarcinoma (chorioepithelioma) Placental site trophoblastic tumor. Types of GTD.

E N D
Types of GTD Benign • Hydatidiform mole/molar pregnancy (complete or incomplete) malignant • Invasive mole • Choriocarcinoma (chorioepithelioma) • Placental site trophoblastic tumor
Types of GTD • The term Gestational Trophoblastic Tumors has been applied the latter three conditions • Arise from the trophoblastic elements • Retain the invasive tendencies of the normal placenta or metastasis • Keep secretion of the human chorionic gonadotropin (hCG)
Pathologic and clinical classifications for gestational trophoblastic disease
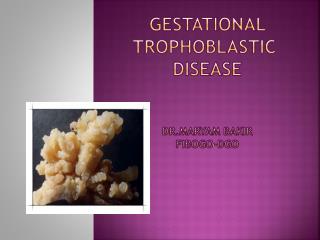
Definition and Etiology • Hydatidiform mole is a pregnancy characterized by vesicular swelling of placental villi and usually the absence of an intact fetus. • The etiology of hydatidiform mole remains unclear, but it appears to be due to abnormal gametogenesis and fertilization
Definition and Etiology • In a ‘complete mole’ the mass of tissue is completely made up of abnormal cells • There is no fetus and nothing can be found at the time of the first scan.
Definition and Etiology • In a ‘partial mole’, the mass may contain both these abnormal cells and often a fetus that has severe defects. • In this case the fetus will be consumed ( destroyed) by the growing abnormal mass very quickly.(shrink)
Incidence • 1 out of 1500-2000 pregnancies in the U.S. and Europe • 1 out of 500-600 (another report 1%) pregnancies in some Asian countries. • Complete > incomplete
Incidence • Repeat hydatidiform moles occure in 0.5-2.6% of patients, and these patiens have a subsequent greater risk of developing invasive mole or choriocarcinoma • There is an increased risk of molar pregnancy for women over the age 40
Incidence • Approximately 10-17% of hydatidiform moles will result in invasive mole • Approximately 2-3% of hydatidiform moles progress to choriocarcinoma ( most of them are curable) Not definitely benign disease , has a tight relationship with GTT
Cytogenetics Complete molar pregnancyChromosomes are paternal , diploid 46,XX in 90% cases 46,XY in a small part Partial molar pregnancyChromosomes are paternal and maternal, triploid. 69,XXY 80% 69,XXX or 69,XYY 10-20% Wrong life message , so can not develop normally
Comparative Pathologic Features of Complete and Partial Hydatidiform Mole
Complete hydatidiform mole demonstrating enlarged villi of various size
The microscopic appearance of hydatidiform mole: • Hyperplasia of trophobasitc cells • Hydropic swelling of all villi • Vessles are usually absent
A sonographic findings of a molar pregnancy. The characteristic “snowstorm” pattern is evident.
Transvaginal sonogram demonstrating the “ snow storm” appearance.
Color Dopplor facilitates visualization of the enlarged spiral arteriesclose proximity to the “ snow storm” appearance
Color Doppler image of a hydatidiform mole and surrounding vessels. The uterine artery is easily identified from its anatomical location.
Dopplor waveform analysis demonstrates low vascular resistance(RI=0.29) in the spiral arteries, much lower than that obtained in normal early pregnancy
Here is a partial mole in a case of triploidy. Note the scattered grape-like masses with intervening normal-appearing placental tissue.
Large bilateral theca lutein cysts resembling ovarian germ cell tumors. With resolution of the human chorionic gonadotropin(HCG) stimulation, they return to normal-appearing ovaries.
Signs and Symptoms of Complete Hydatidiform Mole • Vaginal bleeding • Hyperemesis ( severe vomit) • Size inconsistent with gestational age( with no fetal heart beating and fetal movement) • Preeclampsia • Theca lutein ovarian cysts
Signs and Symptoms of Partial Hydatidiform Mole • Vaginal bleeding • Absence of fetal heart tones • Uterine enlargement and preeclampsia is reported in only 3% of patients. • Theca lutein cysts, hyperemesis is rare.
Diagnosis of hydatidiform mole Quantitative beta-HCG Ultrasound is the criterion standard for identifying both complete and partial molar pregnancies. The classic image is of a “snowstorm” pattern
Diagnosis • The most common symptom of a mole is vaginal bleeding during the first trimester • however very often no signs of a problem appear and the mole can only be diagnosed by use of ultrasound scanning. (rutting check) • Occasionally, a uterus that is too large for the stage of the pregnancy can be an indication. • NOTE: Vaginal bleeding does not always indicate a problem!
Differential diagnosis • Abortion • Multiple pregnancy • Polyhydramnios
Treatment Suction dilation and curettage :to remove benign hydatidiform moles When the diagnosis of hydatidiform mole is established, the molar pregnancy should be evacuated. An oxytocic agent should be infused intravenously after the start of evacuation and continued for several hours to enhance uterine contractility
Treatment • Removal of the uterus (hysterectomy) : used rarely to treat hydatidiform moles if future pregnancy is no longer desired.
Treatment Chemotherapy with a single-agent drug Prophylactic (for prevention) chemotherapy at the time of or immediately following molar evacuation may be considered for the high-risk patients( to prevent spread of disease )
High-risk postmolar trophoblastic tumor • Pre-evacuation uterine size larger than expected for gestational duration • Bilateral ovarian enlargement (> 9 cm theca lutein cysts) • Age greater than 40 years • Very high hCG levels(>100,000 m IU/ml) • Medical complications of molar pregnancy such as toxemia, hyperthyrodism and trophoblastic embolization (villi come out of placenta ) • repeat hydatidiform mole
Follow-up • Patients with hudatidiform mole are curative over 80% by treatment of evacuation. • The follow-up after evacuation is key necessary • uterine involution, ovarian cyst regression and cessation of bleeding
Follow-up • Quantitative serum hCG levels should be obtained every 1-2 weeks until negative for three consecutive determinations, • Followed by every 3 months for 1 years. • Contraception should be practiced during this follow-up period
Definition This term is applied to a molar pregnancy in which molar villi grow into the myometrium or its blood vessels, and may extend into the broad ligament and metastasize to the lungs, the vagina or the vulva.
Invasive mole: the tissue invades into the myometrial layer. No obvious borderline, with obvious bleeding.
A case of invasive mole: inside the uterine cavity the typical “snow storm” appearance can be detected, The location of blood flow suggest an invasive mole.
The same patient owing to the myometrial invasion. Reduced vascular resistance is detected in the uterine artery.
Transvaginal color Doppler scan of a patient with invasive mole Following uterine curettage, Persistent color signals within the myometeriun
Power Doppler easily detects a vascular echogenic nodule within the myometrium, suggesting invasive mole