Download
1 / 54
600 likes | 2.17k Views
Vulvar Cancer. 부산 백병원 산부인과 조인호. Preview. Annually, 3800 new case, 800 deaths in US Uncommon, 3-5% in Gyn cancer 90% of vulvar cancer : Squamous cell ca. Incidence of VIN : 1970 년대 중반 -> 1980 년대 중반 ; 2 배 Invasive squamous cell ca. : stable.

E N D
Vulvar Cancer 부산 백병원 산부인과 조인호
Preview • Annually, 3800 new case, 800 deaths in US • Uncommon, 3-5% in Gyn cancer • 90% of vulvar cancer : Squamous cell ca. • Incidence of VIN : 1970년대 중반 -> 1980년대 중반 ; 2배 • Invasive squamous cell ca. : stable 부산백병원 산부인과
Radical vulvectomy and en bloc groin dissection with or without pelvic lymphadenectomy • Changes in Tx. • Individualization of Tx. For Pt. • Vulvar conservationwith unifocal tumors • Omission of the groin dissection for Pt. with T1 tumors and <1mm of stromal invasion. • Elimination of routine pelvic lymphadenectomy • Separate incisions for the groin dissection to improve wound healing 부산백병원 산부인과
Omission of the contralat. Groin dissection in Pt. with lat. T1 lesions and negative ipsilat. Node. • Preoperative radiation therapy • Postoperative radiation therapy 부산백병원 산부인과
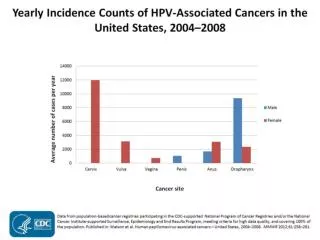
Etiology • Basaloid or warty types • Multifocal, younger, related to HPV infection, VIN, smoking • Keratinizing types • Unifocal, older, not related to HPV infection, adjacent to lichen sclerosus and squamous hyperplasia • VIN3 : potential precancerous lesion • VIN -> cancer ; difficult • VIN (10-20%) ; harbor an invasive component • 80% of VIN found adjacent to basaloid or warty vulvar squamous cell ca. 부산백병원 산부인과
VIN3의 89%, warty or basaloid type carcinos의 86% : DNA of HPV • Itch-scratch cycle associated with lichen sclerosus and squamous hyperplasia, with atypical changes occurring in the repaired epithelium. • Demonstrate aneuploid DNA content, p53 overexpression, and monoclonal expansion of keratinocytes in lichen sclerosus and associated squamous hyperplasia 부산백병원 산부인과
In past, • High risk factor : obese, HBP, DM, nulliparous, • In recent, • Unable to confirm 부산백병원 산부인과
Type of Vulvar cancer • Table 33.1 부산백병원 산부인과
Squamous cell cancer • 90-92% of vulvar cancer • Basaloid carcinoma, warty carcinoma, keratinizing squamous carcinoma • Keratinization • Microinvasive squamous carcinoma • <2cm in diameter /c <1mm stromal invasion • Invasion depth <1mm -> inguinal LN meta : extremely rare • Invasion depth >1mm -> LN meta risk ↑ 부산백병원 산부인과
Squamous cell caClinical Features • Mean age : 65세 (15%는 40세 이전) • Sx. • Vulvar pruritus, a lump, mass • Bleeding, ulcerative lesion, discharge, pain, dysuria • P/Ex. • Raised, fleshy, ulcerated, leukoplakic, warty • Labia majora and minora (60%), clitoris(15%), perineum(10%) • Groin LN examination, Pap smear, colposcopy 부산백병원 산부인과
Squamous cell caDiagnosis • Wedge Bx. • Lesion is 1cm in diameter -> Excision Bx. • Any confluent warty lesion requires biopsy before medical or ablative therapy is initiated 부산백병원 산부인과
Squamous cell caRoutes of Spread • Direct extension to involve adjacent structures • Lymphatic embolization to the regional inguinal and femoral LN • Hematogenous spread to distant sites (lungs, liver, bones) 부산백병원 산부인과
Fig 33.3 부산백병원 산부인과
Staging • Previously, • Clinical staging based on • tumor size • Location • Palpable regional LN • Limited search for distant metastasis • Now, -> Surgical Staging • 18-44% error in clinical staging compared with Surgical Staging 부산백병원 산부인과
Table 33.4 부산백병원 산부인과
Prognosis of survival • Factor • LN status : most important • Lesion size • Histologic grade, tumor thickness, depth of stromal invasion, lymph-vascular space involvement, tumor ploidy • 5-yr survival rate : LN(-) ;90% , LN(+) ;50% • 2-yrs survival rate : • LN meta 3개이상 :20% • N0,N1 : 78%, N2 : 52%, N3 : 33% 부산백병원 산부인과
Table 33.5 부산백병원 산부인과
Table 33.3 부산백병원 산부인과
Treatment • En bloc radical vulvectomy and bilateral dissection of the groin and pelvic nodes • 지난 20년간의 변화 • Early stage (T1) : 50%이상 차지 • Hospitalization의 기간 연장 • Psychosexual consequence에 대한 인식의 증대 부산백병원 산부인과
Early Vulvar Cancer (T1) • The modern approach to the management -> individualized • Microscopic tumor foci가 lymphatics에 남아 있더라도 en bloc resection은 고려하지 않는다. • Radical local excision > Radical vulvectomy • Recurrence, depth of invasion • 1-1.5cm grossly negative margin 부산백병원 산부인과
Patient age -> Tx. 결정 인자 • Lat. or Post. aspects of vulva lesion • >Radical local excision • Clitoris를 침범한경우 -> • Small field of radiation Tx. • Sensitizing chemotherapy 부산백병원 산부인과
T2 , T3 Vulvar cancer • Surgical margin of at least 1cm • More conservative resection • Involving the post. half of the vagina • Preservation of the clitoris and mons pubis • More advanced T2 and T3 • Radical vulvectomy and bilat. inguinal-femoral lymphadenectomy 부산백병원 산부인과
Closure of Large Defects • An area may be left open to granulate, after 6-8 weeks • Full-thickness skin flaps • Rhomboid flap, - post. vulva • Mons pubis pedicle flap – lat. Defects • Myocutaneous flaps • Tensor fascia lata myocutaneous graft 부산백병원 산부인과
Advanced DiseaseLarge T3 and T4 Primary Tumor • Radical vulvectomy and inguinal-femoral lymphadenectomy + pelvic exenteration • Chemoradiation ->90% response (initial) • Op후 chemoradiation 순서 • Radiation alone (/c or /s chemoTx.) • Residual tumor :1/2이상 -> 50-79% relapse • Combined radiation + surgery • 5 yr survival rate : as high as 76% 부산백병원 산부인과
Management of the Lymph Nodes • Groin dissection -> • postop. wound infection • Breakdown • Chronic leg edema (major problem) • Invasion <1mm, no risk of LN metastasis • Recur in undissected groin -> 90% mortality • Lat. Vulvar lesion -> ipsilat. Bilat. Lymphadenectomy becomes necessary • Appropriate groin dissection is the single most important factor in decreasing the mortality 부산백병원 산부인과
Microinvasive Carcinoma • Stromal invasion >1mm ; inguinal-femoral lymphadenectomy • Radiation cannot substitute for groin dissection • Primary lesion is unilateral and the ipsilateral LN are negative -> not necessary to perform a bilateral groin dissection • Groin node (-) -> pelvic node meta is rare • Sentinel LN studies : predict the presence or absence of reginal nodal metastasis 부산백병원 산부인과
Postoperative Management • Inpast, • Bed Rest: 3-5days for immobilization • These days, • Separate incision -> POP 1-2day : ambulation시작 • DVT prevention • Subcutaneous heparin • pneumatic calf compression • Frequent dressing • Suction drainage of each side of the groin • Sitz bath or whirlpool therapy 부산백병원 산부인과
Early Postoperative Comlications • Groin wound infection, necrosis, breakdown • En bloc operation – 53-85% • Separate-incision approach – 44% • UTI • Seromas • DVT • Pulmonary embolism • MI • Hemorrhage 부산백병원 산부인과
Late Complications • Chronic lymphedema (30%) • Recurrent lymphagitis or cellulitis (10%) • Usually responds to oral antibiotics • SUI (10%) • Femoral hernia (uncommon) • Depression, altered body image and sexual dysfunction 부산백병원 산부인과
Role of Radiation Therapy • RTx : 점점 중요한 요소로 부각됨 • Local tissue tolerance : poor, vulvar necrosis • Ix. for RTx. with primary vulvar ca. • Advanced disease • Op.후 LN meta가 microscopic하게 2개 이상 (+), gross하게 1개이상 (+) • Possible roles for RTx. • Involved or close surgical margin인 경우 • Small primary tumor인 경우 primary Tx., • Particularly clitoral or periclitoral lesion • Op할 경우 Psychologic한 결과가 예상되는 경우 부산백병원 산부인과
1 microscopically positive groin node (+) -> No additional Tx. Recommended • Microscopic groin node 2개 이상 (+) -> recurrence risk ↑ • =>irradiation • The survival rate (1977, GOG positive groin (+)) 부산백병원 산부인과
Recurrent Vulvar cancer • 2/3 of vulvar cancer recur within first 2years from initial Tx. • Positive groin nodes와 recurrence는 정비례 • Local recurrence • Margin status • Closer than 0.8cm -> 50% recur • Primary lesion larger than 4cm in diameter • Tx. • Additional surgery • RTx (External beam therapy + interstitial needles) • chemotherapy 부산백병원 산부인과
Regional and Distant Recurrence • Difficult • Poor prognosis • Radiation • Chemotherapy • Bleomycin and methotrexate with or without cisplatin • Bleomycin and mitomycin C • Response • Usually disappointing • Long-term survival is very uncommon 부산백병원 산부인과
Melanoma • Rare • Incidence : 0.1~0.19/100,000women • Second most common of vulvar malignancy • Postmenopausal white women • No symptoms (most) • Itching, bleeding, groin mass • Labia minora, clitoris • Vulvar nevi are junctional, precursor lesion to melanoma; thus, should be removed 부산백병원 산부인과
Melanoma Histopathology • Mucosal lentiginous melanoma • Flat freckle, quite extensive, superficial • Superficial spreading melanoma • Most common, superficial • Nodular melanoma • Most aggressive, raised lesion • Penetrate deeply • Metastasize widely • ¼ of cases of melanomas • Macroscopically amelanotic -> spread early 부산백병원 산부인과
Melanoma Staging • The FIGO staging used for squamous lesions is not applicable to melanomas • Because the lesions are usually much smaller, • and the prognosis is related to the depth of tumor invasion rather than to the diameter of the lesion 부산백병원 산부인과
Melanoma Treatment (1) • Understanding of the prognostic significance of the microstage • Individualization • More conservative surgical management • Invasion 에 따른 Tx.방침 • (<1mm) : Radical local excsion alone • (>1mm) : en bloc resection of the primary tumor and regional groin node dissection recommended • 1cm이상 surgical margin (<0.76mm) • 2cm이상 surgical margin (1-4mm) 부산백병원 산부인과
Melanoma Treatment (2) • 10-year survival rate • Lateral lesion (61%), medial lesion (37%) • Superfical lesion (Breslow tumor thickness <0.76mm ) • Lymphadenectomy not indicated • Intermediate-thickness (1-4mm) • Observation showed a 5-year survival advantage who underwent lymph node dissection • Deeply invasive cutaneous melanoma (>4mm) • Benefit from regional lymphadenectomy • Chemotherapy : interferon -a 부산백병원 산부인과
Melanoma Prognosis 부산백병원 산부인과