Download

1 / 37

E N D
BIOLOGY OF TOOTH MOVEMENT Presented by: Presented by: Omara Omara Albert Martin Albert Martin BDS(EQUSaT EQUSaT), ), Phdo Phdo(IPI DEAsbl DEAsbl(Aesthetic Dentistry) (Aesthetic Dentistry) BDS( (IPI- -Maya), Maya), +256777220490, +256758144276
Introduction Orthodontic tooth movement is a unique process where a solid object (tooth) is made to move through a solid medium (bone). The ability of independent movement of the teeth is unique to humans in particular and mammals In general as teeth are not ankylosed to the bone.
Orthodontic treatment is possible due to the fact that whenever a prolonged force is applied on a tooth, bone remodeling occurs around the tooth resulting in its movement. Bone subject to pressure as a result of compression of periodontal ligament resorbs while bone forms under tensile force as a result of stretching of the periodontal ligament.
Physiologic Tooth Movement They are naturally occurring tooth movements. . Physiologic tooth movements include : ➢A. Tooth eruption. ➢B. Migration or drift of teeth. ➢C. Changes in tooth position during mastication.
➢Tooth Eruption Tooth eruption is the axial movement of the tooth from its developmental position in the jaw to its final position in the oral cavity.
Theories of tooth eruption A. Blood pressure theory : The tissue around the developing end of the root is highly vascular, this vascular pressure is believed to cause the axial movement. B. Root growth: The apical growth of roots results in an axially directed force that brings about the eruption of the teeth .
C. Hammock ligament: A band of fibrous tissue exists below the root apex and Is rich in fluid droplets. The developing root forces itself against this band of tissue, which in turn applies an occlusally directed force on the tooth. D. Periodontal ligament traction: The periodontal ligament is rich in fibroblasts that contain contractile tissue. The contraction of these periodontal fibers (mainly oblique group of fibers) result in axial movement of the tooth.
➢Migration Or Drift Of Teeth It is the minor changes in tooth position observed after eruption of teeth. In case of the maxillary dentition, it shows a natural tendency to move in a mesial and occlusal direction. As the teeth undergo occlusal and proximal wear, they move in a mesial and occlusal direction to maintain inter-proximal and occlusal contact.
➢Tooth movement during mastication The teeth and periodontal structures are subjected to intermittent heavy forces which occur in cycles of one second or less and may range from 1- 50 kilograms . A tooth subjected to these heavy forces, exhibits slight movement within its socket and subsequently returns to its original position .
Histology Of Tooth Movement The histological changes seen during tooth movement vary according to the amountand duration of force applied, its classified as: A. Changes following application of mild force. B. Changes following application of extreme force.
A.Changes Following Application Of Mild Force When a force is applied to a tooth, areas of pressure and tension are produced. Changes on pressure side : 1. The periodontal ligament in the direction of the tooth movement gets compressed to almost l/3rd of its original thickness. 2. Increase in Cellular proliferation within a few days .
3. Osteoclasts migrate into the PDL from blood vessels . 4. When the forces applied are within physiologic limits, the resorption is seen in the alveolar plate immediately adjacent to the ligament. This kind of resorption is called frontal resorption.
Changes on tension side : 1. Stretching of PDL fibres the distance between the alveolar process and the tooth is widened. 2. Cellular proliferation of fibroblasts and osteoblasts . 3. Deposition of osteoidimmediately adjacent to the lamina dura.
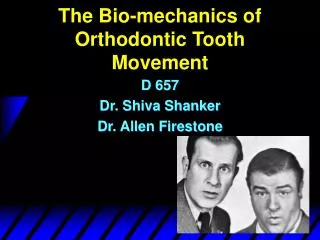
4. Secondary remodeling changes take place elsewhere to maintain the width or thickness of the alveolar bone. ❖If a tooth is being moved in a labial direction, there is compensatory deposition of new bone on the outer side of the labial alveolar bony plate and a compensatory resorption on the lingual side of the lingual alveolar bone .
A. Secondary remodeling changes seen following the application of a bodily force in a lingual direction . B. Secondary remodeling changes seen following the application of a tipping force in a lingual direction .
Tension side Pressure side
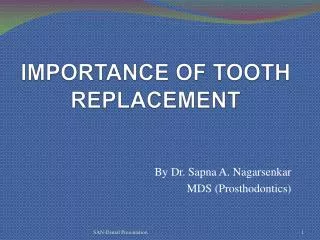
B.Changes Following Application Of Extreme Force On the pressure side : 1. Capillary blood vessels are crushed resulting in death of cells in PDL (hyalinization(. 2. In areas adjacent to the hyalinized sections of PDL cellular proliferation occurs . 3. Resorption occurs deep to hyalinized area from cancellous bone outwards toward lamina dura of PDL (undermining resorption(.
On the tension side : 1. The periodontal ligament gets over-stretched leading to tearing of the blood vessels and ischemia. 2. Increase in osteoclastic activity as compared to bone formation with the result that the tooth becomes loosened in its socket.
Diagram showing the effect of applying an excessive force Areas of hyalinization (1( Undermining resorption (2( Direct resorption in areas where force is less (3(
Optimum Orthodontic Force It is one which moves teeth most rapidly in the desired direction, with the least possible damage to tissue and with minimum patient discomfort. the optimum force is equivalent to the capillary pulse pressure which is 20-26 gm/ sq.cm of root surface area.
It has the following characteristics: 1. Produces rapid tooth movement. 2. Minimal patient discomfort . 3. The lag phase of tooth movement is minimal. 4. No marked mobility of the teeth being moved. 5. The vitality of the tooth and supporting periodontal ligament Is maintained. 6. Initiates maximum cellular response and Produces direct or frontal resorption .
Phases Of Tooth Movement Tooth movement progresses through three stages : A. Initial phase : 1. Very rapid tooth movement is observed over a short distance which then stops . 2. It represents displacement of the tooth in the periodontal membrane space and probably bending of alveolar bone to a certain extent. 3. The tooth movement in the initial phase is between 0.4 to 0.9 mm and usually occurs in a week's time.
B. Lag phase : 1. During this phase, little or no tooth movement occurs. 2. Characterized by formation of hyalinized tissue in the periodontal ligament which has to be resorbed before further tooth movement can occur . 3. If light forces are used, the area of hyalinization is small and frontal resorption occurs. 4. If heavy forces are used, the area of hyalinization is large. Resorption in this case is undermined and a longer lag period occurs lo eliminate the hyalinized tissue.
5. The lag phase usually extends for 2-3 weeks but may at times be as long as 10 weeks. C. Post lag phase : 1. After the lag phase, tooth movement progresses rapidly as the hyalinized zone is removed and bone undergoes resorption.
Theories Of Tooth Movement A. Pressure tension theory by Schwarz . B. Blood flow theory by Bien . C. Bone bending piezoelectric theory .
Reasons For More Rapid Tooth Movement In Children Physiological tooth movement is greatest when the teeth are erupting . The periodontal ligament is more cellular, and therefore there are more cells available for resorption and remodeling The alveolar bone has a greater proportion of osteoblasts The cellular response in reaction to an applied force is quicker
The width of the periodontal ligament is increased in newly erupted teeth, and so a greater force can be applied before constriction of the blood vessels occurs . Growth can be utilized .
Drugs And Tooth Movement The rate of orthodontic tooth movement can be altered by applying certain drugs locally or systemically. A. Promoter drugs These agents basically enhance bone resorption . They couple with the secondary and primary inflammatory mediators and enhance tooth movement .
They are : 1. Prostaglandin’s 2. Leucotriens 3. Cytokines 4. Vitamin d 5. Osteocalcin 6. Corticosteroids Except vitamin d and corticosteroids the other above said agents are not that much widely used in medical profession.
Since bone turn over rate will be more for those patients under any of the above said drugs, care should be taken by utilizing low forces or by giving increased duration between appliance activation appointments. The duration of orthodontic treatment is usually 18 months, this extended duration can be reduced by applying promoter agents locally near the moving unit, (i.e. anteriors)
B.Suppressor agents These agents basically reduce bone resorption . 1. Nonsteroidal anti-inflammatory agents -- they interfere with archidonic acid metabolism, blocks production of primary and or secondary messengers. ❖Since NSAIDs are freely available over the counter, patients should be advised not to take these drugs during orthodontic treatment, without the dentist’s knowledge.
2. Bisphosphonates – bind with calcium ions, promotes apoptosis of working osteoclasts. ❖The bisphosphonate groups of drugs are economically more in cost and not easily available over the counter, but they are the drugs of choice for patients with osteoporosis. ❖A thorough medical history will definitely reveal whether the patient is under such a treatment, caution should be taken while taking up these patients for orthodontic treatment
❖At present orthodontic mini implants are used to aid in anchorage, when compared to headgears which also aid in anchorage these implants costs more. Moreover most of the patients deny wearing headgears. ❖Alternatively the suppressor agents can be delivered locally near the anchor unit (i.e. molars) to enhance anchorage and retention.
References...for further studies (@omara_albertm)