Download
1 / 44
440 likes | 590 Views
Robert L Worthington-Kirsch, MD, FSIR, FCIRSE, RVT, RPVI. Randomized Trial of Bead Block TM vs Embosphere TM for UAE for Fibroids. This study is supported by an unrestricted grant from Biocompatibles and Terumo

E N D
Robert L Worthington-Kirsch, MD, FSIR, FCIRSE, RVT, RPVI Randomized Trial of Bead BlockTM vs EmbosphereTM for UAE for Fibroids
This study is supported by an unrestricted grant from Biocompatibles and Terumo • Dr Worthington-Kirsch is an active consultant to Biocompatibles, Terumo, Biosphere Medical, and Vascular Solutions Disclosures
UAE has been established as mainstream therapy for fibroid disease • Embolic choice evolving • Calibrated hydrogel spheres preferred • Tris-acryl/gelatin most commonly used • PVA hydrogel is an emerging alternative Background
Very similar to soft contact lenses • PVA has been used as implanted biomaterial since the 1940s • Very different properties than non-hydrogel PVA preparations PVA Hydrogel Spheres
Clinical experience suggests that BB as effective as ES for UAE • Requires proper technique • Randomized trial needed to confirm or disprove anecdotal experience Study Rationale
Non-inferiority • 22 patients per arm gives desired power • PRCT (Level I data) • Patients not informed about embolic used • MRI grader blinded for embolic used • Reviewed/approved by FDA Study Design
Similar to other UAE studies • Women ages 30-50 • Symptomatic fibroids without other uterine disease • Uterus >250cc, <24 weeks Admission Criteria
MRIs on designated magnet • Pre-UAE, 3-7 days post-UAE, 3 months, 6 months • Best protocol for each embolic • BB – start with 700-900 • ES – start with 500-700, unless Ovarian A seen • Terumo Progreat microcatheter • Consistent defined embolization endpoints Study Design
New filling of Ovarian A or cross-uterine collaterals • Retrograde flow around catheter tip • “Plumping” of artery with injection • No further filling of ascending branch Embolization Endpoints
MRI fibroid perfusion • “immediate”, 3 months, 6 months • Uterine/dominant fibroid size • UFS-QOL • 3 months, 6 months, 1 year Outcome Measures
2 cohorts • Site 1 – 22 patients • Complete follow-up data set • 1 technical failure (anatomic basis) • Site 2 – 22 + 2 patients • 1 withdrawal from initial 22 • Follow-up complete except for 12 month QOLs • 22 analyzable patients in each arm Study to Date
No serious complications • All UAEs clinically successful per patients • Including technical failure • 3 “failures” to discuss in more detail Study to Date
1 Week post-UAE (MRI only) – 43/44 (97%, 1 ES) • 3 Mo post-UAE • MRI – 36/44 (82%, 5 ES, 3 BB) • QOL – 39/44 (88%, 3 ES, 2 BB) • 6 Mo post-UAE • MRI – 37/44 (84%, 4 ES, 3 BB) • QOL – 43/44 (97%, 1 BB) • 12 Mo post UAE (QOL only) – 21/21 Study to Date – Follow Up
Pre-UAE perfusion scored at 10 • Global fibroid burden, not just dominant fibroid • Follow-up perfusion scored 1-10 • 1 – Complete infarction all visible fibroids • 1-2 - “Success” (10% or less residual perfusion) • 3-4 – “Partial Success” (11-30% residual perfusion) • 5 or higher - “Failure” (>30% residual perfusion) MRI Grading
Symptom Score, QOL Score. QOL Subscales • Change of 10 points or greater significant UFS-QOL Grading
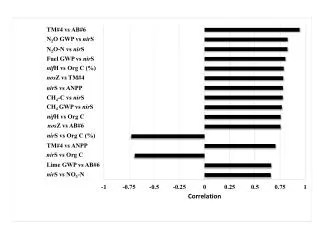
Bead Block Embosphere QOL Subscales
Patient # 2-003 • Embosphere • Complete infarction at 1 week and 3 months • Significant reperfusion (4) at 6 months • SS 94>44>0 • QOL 86>89>96 • Will symptoms recur? Treatment Failures?
Patient # 2-016 • Bead Block • Almost complete infarction (2) on all f/u MRIs • SS 41>69>66 (worsening) • QOL 66>50>52 (borderline improvement) Treatment Failures?
Patient # 2-013 • Embosphere • Perfusion score 3 @ 1 week, then 2 • SS 47>25>31 • QOL 53>56>51 Treatment Failures?
General consensus in literature is that UAE failure rate is ~10%. • 3 Failures out of 44 patients is not unexpected. Treatment Failures?
Well–defined inclusion/exclusion criteria • Adequate sample size/power analysis • Randomization by independent third party • Double-blinding • Identical care and follow-up Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteria • Adequate sample size/power analysis • Randomization by independent third party • Double-blinding • Identical care and follow-up Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteria • Adequate sample size/power analysis • Randomization by independent third party • Double-blinding • Identical care and follow-up Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteria • Adequate sample size/power analysis • Randomization by independent third party • Double-blinding • Identical care and follow-up Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteria • Adequate sample size/power analysis • Randomization by independent third party • Double-blinding • Identical care and follow-up Spies – “How to Evaluate New Embolics”
Well–defined inclusion/exclusion criteria • Adequate sample size/power analysis • Randomization by independent third party • Double-blinding • Identical care and follow-up Spies – “How to Evaluate New Embolics”
Intention to treat analysis • Blinded imaging assessment • Clear endpoint assessment • UFS-QOL, Enhanced MRI • Reporting Spies – “How to Evaluate New Embolics”
Intention to treat analysis • Blinded imaging assessment • Clear endpoint assessment • UFS-QOL, Enhanced MRI • Reporting Spies – “How to Evaluate New Embolics”
Intention to treat analysis • Blinded imaging assessment • Clear endpoint assessment • UFS-QOL, Enhanced MRI • Reporting Spies – “How to Evaluate New Embolics”
Intention to treat analysis • Blinded imaging assessment • Clear endpoint assessment • UFS-QOL, Enhanced MRI • Reporting Spies – “How to Evaluate New Embolics”
Intention to treat analysis • Blinded imaging assessment • Clear endpoint assessment • UFS-QOL, Enhanced MRI • Reporting Spies – “How to Evaluate New Embolics”
Intention to treat analysis • Blinded imaging assessment • Clear endpoint assessment • UFS-QOL, Enhanced MRI • Reporting Spies – “How to Evaluate New Embolics”