Got Aldosterone?
Got Aldosterone?. Aldosterone Synthesis. Aldosterone is produced in the zona glomerulosa of the adrenal gland The enzyme aldosterone synthase encoded by the gene CYP11B2 gene converts deoxycorticosterone to aldosterone via a series of steps

Got Aldosterone?
E N D
Presentation Transcript
Aldosterone Synthesis • Aldosterone is produced in the zona glomerulosa of the adrenal gland • The enzyme aldosterone synthase encoded by the gene CYP11B2 gene converts deoxycorticosterone to aldosterone via a series of steps • In glucocorticoid remediable aldosteronism (GRA), a chimeric gene containing the promotor sequence of CYP11B1 and functional elements of CYP11B2 is created, resulting in aldosterone production under the control of ACTH
Mineralocorticoid Receptor (MR) • Aldosterone acts by diffusing into cells and attaching to a specific receptor, mineralocorticoid receptor (MR) in the cytosol which then leads to the synthesis of new proteins called aldosterone-induced proteins (AIPs). • Cortisol binds to the MR receptor at equal affinity and is found in much higher concentrations then that of aldosterone. However target cells contain 11ß-hydroxysteroid dehydrogenase that converts cortisol to cortisone which is inactive. • If 11ß-hydroxysteroid dehydrogenase is inactivated, such as in the syndrome of apparent mineralocorticoid excess, or inhibited such as occurs in chronic ingestion of licorice patients can present with findings similar to hyperaldosteronism. • MR are found in high concentrations in the renal distal nephron as well as the colon and sweat and salvary glands, but also has been found in the heart, brain, vascular smooth muscle, liver, and blood leukocytes
Action on Renal Tubular Cells • Aldosterone promotes the reabsorption of NaCl and the secretion of K+ in the principal cells in the cortical collecting tubules • The intercalated cells in the cortex contain MR and aldosterone enhances H+ secretion via H+-ATPase pumps in the apical membrane. • Na+ reabsoprtion via the principal cells causes a lumen-negative potential which causes an electrical gradient favorable for H+ accumulation • Aldosterone also enhances NaClreabsorption in the distal tubule by increasing the number of Na+-Cl- cotransporters in the luminal membrane
Aldosterone increases the number of open Na+ and K+ channels in the luminal membrane Increases activity of the Na+-K+-ATPase pump in the basolateral membrane The AIP, serum glucocorticoid-regulated kinase (sgk), increased number of ENaC channels on the surface Nedd4 inhibits ENaC; Sgk reduces interaction of Nedd4 and ENaC The movement of Na+ through its channel ENaC is electrogenic, creates a lumen-negative potential difference. Electroneutrality is maintained in this setting either by passive Cl- reabsorption via the paracellular pathway or by K+ secretion from the cell into the lumen
Inhibition and Stimulation • Aldosterone is stimulated by a number of factors but the most important include angiotensin II, hyperkalemia, and ACTH. • Angiotensin II and hyperkalemia stimulate both the synthesis and stimulation of aldosterone synthase in the zona glomerulosa. • Aldosterone inhibition occurs predominantly by ANP and hypokalemia
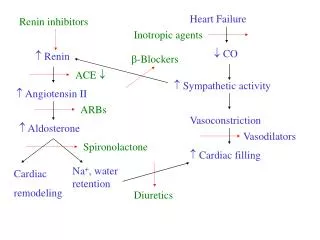
It has been suggested that aldosterone regulates blood pressure through a number of mechanisms.
Aldosterone and Hypertension • Primary aldosteronism as described by Conn in 1955 had been thought to be an uncommon cause of hypertension with prevalence of < 1% among hypertensive patients • Gordon et al in early 1990s screened 52 hypertensive pts and found that 12% of the individuals were positive for primary aldosteronism • In a follow up study by Gordon evaluation of 199 pts referred to a hypertension clinic found a prevalence of primary aldosteronism to be at least 8.5%
Aldosterone and Hypertension • Since the early studies by Gordon multiple investigators have confirmed a prevalence of primary aldosteronism of 5-15% in general selective hypertensive population. Two studies in particular: • Schwartz and Turner evaluated 118 pts with hypertension and withdrew antihypertensive treatment. Diagnosis of primary aldosteronism was made with 4 day salt load and lack of suppresion of aldosteronesecreation • Primary aldosteronism was diagnosed in 13% of individuals
Aldosterone and Hypertension • Mosso et al. took > 600 hypertensive patients and screened them for primary aldosteronism by measurements of plasma aldosterone/PRA ratio • Pts with high ratio were evaluated by fludrocortisone suppresion testing to confirm the diagnosis of primary aldosteronism • Overall the prevalence of primary aldosteronism was 6.1% but increased with relation to the severity of hypertension
Stage 1 140-159/90-99 Stage 2 160-179/100-109 Stage 3 >180/110
Studies from separate laboratories suggest that primary aldosteronism is a common cause of resistant hypertension, with prevalence of approximately 20% • 75% of pts in the Birmingham study had suppressed renin activity despite all pts were on a diuretic and ACEI or ARB • 67% of pts in the Oslo study had supressed renin activity also despite use of diuretics and ACEI or ARB. • This suggests mineralocorticoid excess beyond the 20% of pts who were identified to have true primary aldosteronism
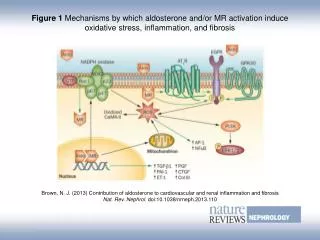
Aldosterone and Kidney Fibrosis • Aldosterone’s ability the enhance systemic and intraglomerular capillary pressure has been favored as the major mode of damage to the kidney • However recent animal studies suggest that aldosterone may have a more direct effect on the kidneys. • In other organs such as the heart it has already been shown that after MI excessive aldosterone production is associated with harmful local effects that lead to fibrosis • Aldosterone infusion in adrenalectomized rats with renal mass ablation (a model of progressive kidney disease) cancels the renoprotective effects of ACEI or ARBs.
Aldosterone and Kidney Fibrosis • In vitro studies show aldosterone increased TGF-B and fibronectin production by mesangial cells in culture • Aldosterone infusion for 3 days in normal rats cause more than 2 fold increase in urinary excretion of TGF-B • TGF-B signaling pathways upregulate collagen synthesis and promote fibroblast proliferation
Aldosterone and Kidney Fibrosis • Some of the effects of TGF-B are mediated by connective tissue growth factor (CTGF) • CTGF stimulate proliferation of renal fibroblasts and induce extracellular matrix synthesis • It has been shown in vitro that aldosterone significantly increases CTGF gene expression and protein synthesis in cultured mesangial and proximal tubular cells
Aldosterone and Kidney Fibrosis • In rats adosterone has been shown to increase reactive oxygen species (ROS) and other proinflammatory cytokines • ROS has been shown to induce proximal tubular cell apoptosis as well as expansion of mesangial matrix and enhanced cell proliferation
Aldosterone and Kidney Fibrosis • Plasminogen activator inhibitor-1 (PAI-1) is known to promote accumulation of extracellular matrix in endothelial cells • Several studies have shown that aldosterone causes that up-regulation of PAI-1 expression independent of TGF-B or ROS production.
Aldosterone and Kidney Fibrosis • Spironolactone limits the development of glomerulosclerosis in tubulointerstitial fibrosis in rats with streptozotocin induced diabetic nephropathy • In Dahl salt sensitive rats, a model of hypertensive glomerulosclerosis, eplerenone prevents podocyte damage, proteinuria, and glomerulosclerosis • Inihibition of aldosterone receptor also has shown in rat models to provide renoprotection in animals with established renal injury