Download
1 / 39
430 likes | 722 Views
Understand the pathology, clinical symptoms, and diagnosis of rheumatic fever, a serious condition following streptococcal infection. Learn the predisposing factors and treatment approaches.

E N D
Rheumatic Fever Prof. Lotfy Hamed Abo dahab. Professor Of Internal Medicin. Faculty Of Medicin Sohag University.
Rheumatic FeverAet:RF always follows throat infection by a group A hemolytic streptococci e.g.tonsilitis,……..Almost one third of the pt. with acute RF deny the occurrence of antecedent throat infection.Streptococcus hemoliticus type A has in its surface antigens structurally simillar to the glycoprotein of the cardiac valves and the synovial memmbrane of the joints.Following streptococcal infection, the body starts to form antibodies against these streptococcal antigens which react with the cardiac and synovial tissue producing carditis, arthritis,…….
Pathology and Pathogenesis:Acute rheumatic fever is characterized by exudative and proliferative lesions in connective tissue The specific microscopic lesion of RF is Perivascular granulomatous reaction and vasculitis “Aschoff body”.The lesions occurs mainly in relation to heart valves, and the pericardium.* The valve cusps become thickened by odema and infiltration and vegitations are formed on them .the most commonly affected valves are mitral, aortic and rarely tricusped or pulmonary. * A thickened and roughened area (MacCallum’s patch) is frequently present in the left atrium . .
* Foci of coronary arteritis – diffuse vaculitis (aneurysms and thrombosis are not typical features) . * Pericardial affection results in thickening of the pericardium and may be fibrinous effusion.Chronic RHD results from either valvular damage produced by the inflammatory process or from fibrosis occuring during healing* Arthritis of acute RHD is charaterized by a fibrinous exudate and sterile effusion without erosion of the joint surfaces * The subcutaneous nodules have the histologic features of Aschoff nodules
Predisposing factors:1-Epidemiology of RF is the same as the epidemiology of streptococcal throat infection: more prevelant in poor ,undernurished communities, living in overcrowded unhygienic homes, more in winter.2-RF affects mainly children 5-15 years.3-Recurrence rate is very high.4-Both sexes are equally affected but R chorea is more common in females.
Clinical picture:The dis. Usually starts 2-3 weeks after the onset of acute beta hemolytic streptococcal infection
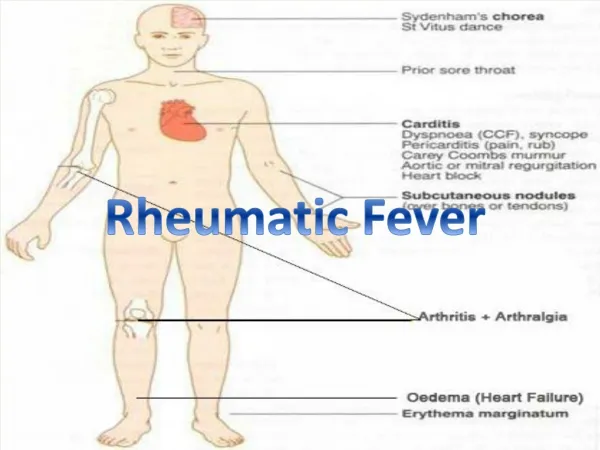
1-Arthritis:- It is the most common manifestation-It affects the big joints -Migratory-No permenant joint affection-Less marked in children and more severe in adults.-Articular signs and symptoms disappear very rapidly with salicylate therapy.Growing pain in and around the joints and the muscles may be a symptom of RF”arthralgia”.2-Carditis:- -It is more common in children than adults-It may present as:A-Pericarditis:-It may be dry resulting in stitching pain in the pericordium . increases with respiration, and a pericardial rub.It may be associated with effusion w. is usually small.
B-Myocarditis: Is manifested by :1-Tachycardia out of proportion to fever2-Dilation in the heart (HF).3-Dilation in the AV rings may result in mitral or tricuspedregurge.4-Muffled HSs, and gallop rhythm.5-Prolonged P-R intervals in the ECG.C-Endocarditis: Affecting the heart valves.-(Carey-Coombs murmur) w. is a transient diastolic murmur heared over the mitral area due to odema, swelling and stifness of the MV, and it disappear when the acute phase resolves.-Destruction and deformition of the mitral and aortic valves lead to permenant MR, AR, MS or AS.
3-Sydenham`s Chorea:- Is due to involvement of the basal ganglia by the rheumatic process.-It occurs mainly in females.-It is usually a late manifestation and may occur after all other rheumatic signs have been subsided, and may occur as the only evidence of rheumatic activity even with normal laboratory findings.-It consists of abnormal semipurposeful movements of the limbs, face and the tongue,…………4-Evidence of past streptococcal infection:-History of sore throat-Antistreptolysin O (w. is an antibody against a lysin enzyme produced by streptococci.
5-Systemic manifestations:-Fever,and profuse sweating-Pallor, anorexia.High ESR, C reactive protein-Anemia and Increase WBCs.6-Subcutaneous nodules: W. are collections of “Aschoff” bodies found over the bony prominences and in tendon sheaths. They are not tender and the skin covering is freely mobile.-They are rare and when they are present they are char. to RF with carditis.
7-Erythema marginatum: These are pink patches appear mainly on the trunck and their margins are slightly raised and are pathognomonic to RF
8-Less common features: -Rheumatic pnumonia, -Epistaxis -Plurisy -Abdominal pain due to vasculitis of internal organs.Diagnosis:.Jones criteria of RF:i-Major criteria: II-Minor criteria1-Polyarthritis 1-Fever 2-Carditis 2-Arthralgia3-Chorea 3-High ESR4-SC nodules 4-+ve C-reactive protein5-Erythema marginatum 5-Prolonged PR intervalThe diagnosis of RF cannot be made except in the presence of at least one major criteria plus two minor criteria (or two major ) in the presence of evidence of previous strep. infection
Prevention;1-primary preventionPreventing the streptococcal infection by: -Improving the socio-economic conditions. -Early treatment of streptococcal throat infection by procaine penicillin 600,000 unit IM for 12 days . benzathine penicillin 1,200,000 unit Im once to eradicate all traces of streptococci. Pts. Who are allergic to penicillin should receive erythromycin 1gm daily for 10 days.Tonsillectomy: is not routinely indicated. It should be done only if there is recurrent attacks of acute tonsillits each year or in cases of chronic septic tonsillitis that cannot adequately controlled by antibiotic therapy.
2-Secondry preventionAll those with a previous attack of RF are in danger “high recurrence rate”. They must be given long acting prophylaxis by long acting benzathin penicillin IM, 1,200,000 units for adults and 600,000units for children every 3-4 weeks.Pts. Who allergic to penicillin should receive sulfadiazine 1gm daily, or erythromycin 250mg twice daily. The duration of prophylaxis should be individualized.
Treatment:1-Rest in bed until all signs of activity disappears. The best clinical criteria for improvement are sleeping pulse, and ESR. Early ambulation may result in recurrence.Low nutrition diet must be given to the pt. and if carditis present low salt diet must be given to the pt.2-Penicillin:to eradicate all traces of streptococcal infection 600,000units of procaine penicillin IM for 10 days or 1,2 million of benzathine penicillin IM once.
3-Salicylates: Are the drug of choice when there is no carditis. Acetyl salcylic acid 4-6 gm are given every day in divided doses depending on age and body weight. It results in prompt disappearance of fever and arthritis but the incidence of eventual development of chronic valvular disease is not affected.The full dose of salicylates should be continued for at least 10 days after disappearance of all clinical manifestation of activity, then reduced to 2/3 dose and continued till all laboratory manifestations of inflammatory disease is returned to normal.
4-Steroids: The effects of steroids are the same as those of salicylates.Steroids are used instead of salicylates in the following situations: -Cases of severe carditis -Cases who are not responding to salic. -Cases allergic to salic.Prednisone 40-60 mg are given per day until the disappearance of fever toxemia and arthritis and then reduce gradually and stopped when the ESR returns to normal. Salicylates should be given during withdrwal of steroids and continued for at least 4 weeks after their cessation in order to prevent recurrences.
5-Chorea:. -Keep in quiet enviroment- -Sedation by diazepam, chloropromazine, haloperidol, or sodium valporate.6-Treatment of complications:.Heart failure is treated in the usual way. As steroids cause water retention w. aggravates failure, diuretics with K supplement should be given. Pericarditis is treated with analgesics for pain and steroids for inflammation. Pericardiocentesis to relieve tamponade is rarely necessary