Download
1 / 61
610 likes | 1.35k Views
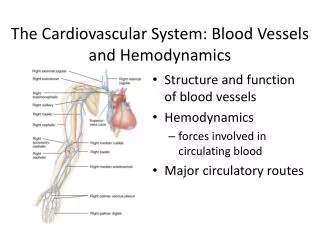
2. INTRODUCTION. Hemodynamics is the means by which blood flow is altered and distributed and by which blood pressure is regulated.. 3. The Cardiovascular System: Blood Vessels and Hemodynamics. Structure and function of blood vesselsHemodynamicsforces involved in circulating bloodMajor circulatory routes.

E N D
1. 1 Chapter 21 The Cardiovascular System:
Blood Vessels and Hemodynamics
2. 2 INTRODUCTION Hemodynamics is the means by which blood flow is altered and distributed and by which blood pressure is regulated.
3. 3 The Cardiovascular System: Blood Vessels and Hemodynamics Structure and function of blood vessels
Hemodynamics
forces involved in circulating blood
Major circulatory routes
4. 4 STRUCTURE AND FUNCTION OF BLOOD VESSELS Angiogenesis: the growth of new blood vessels
It is an important process in the fetus and in postnatal processes
Malignant tumors secrete proteins called tumor angiogenesis factors (TAFs) that stimulate blood vessel growth to nature the tumor cells
Scientists are looking for chemicals that inhibit angiogenesis to stop tumor growth and to prevent the blindness associated with diabetes.
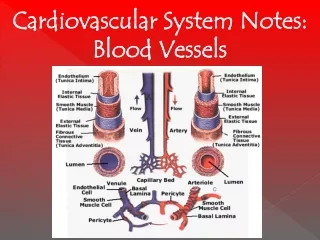
5. 5 Vessels Blood vessels form a closed system of tubes that carry blood away from the heart, transport it to the tissues of the body, and then return it to the heart.
Arteries carry blood from the heart to the tissues.
Arterioles are small arteries that connect to capillaries.
Capillaries are the site of substance exchange between the blood and body tissues.
Venules connect capillaries to larger veins.
Veins convey blood from the tissues back to the heart.
Vaso vasorum are small blood vessels that supply blood to the cells of the walls of the arteries and veins.
6. 6 Arteries The wall of an artery consists of three major layers.
Tunica interna (intima)
simple squamous epithelium known as endothelium
basement membrane
internal elastic lamina
Tunica media
circular smooth muscle & elastic fibers
Tunica externa
elastic & collagen fibers
7. 7 Arteries Arteries carry blood away from the heart to the tissues.
The functional properties of arteries are elasticity and contractility.
Elasticity, due to the elastic tissue in the tunica internal and media, allows arteries to accept blood under great pressure from the contraction of the ventricles and to send it on through the system.
Contractility, due to the smooth muscle in the tunica media, allows arteries to increase or decrease lumen size and to limit bleeding from wounds.
8. 8 Sympathetic Innervation Vascular smooth muscle is innervated by sympathetic nervous system
increase in stimulation causes muscle contraction or vasoconstriction
decreases diameter of vessel
injury to artery or arteriole causes muscle contraction reducing blood loss (vasospasm)
decrease in stimulation or presence of certain chemicals causes vasodilation
increases diameter of vessel
nitric oxide, K+, H+ and lactic acid cause vasodilation
9. 9 Elastic Arteries Large arteries with more elastic fibers and less smooth muscle are called elastic arteries and are able to receive blood under pressure and propel it onward.
They are also called conducting arteries because they conduct blood from the heart to medium sized muscular arteries.
They function as a pressure reservoir.
10. 10 Muscular Arteries Medium-sized arteries with more muscle than elastic fibers in tunica media
Capable of greater vasoconstriction and vasodilation to adjust rate of flow
walls are relatively thick
called distributing arteries because they direct blood flow
11. 11 Arterioles Arterioles are very small, almost microscopic, arteries that deliver blood to capillaries.
Through vasoconstriction (decrease in the size of the lumen of a blood vessel) and vasodilation (increase in the size of the lumen of a blood vessel), arterioles assume a key role in regulating blood flow from arteries into capillaries and in altering arterial blood pressure.
12. 12 Arterioles Small arteries delivering blood to capillaries
tunica media containing few layers of muscle
Metarterioles form branches into capillary bed
to bypass capillary bed, precapillary sphincters close & blood flows out of bed in thoroughfare channel
vasomotion is intermittent contraction & relaxation of sphincters that allow filling of capillary bed 5-10 times/minute
13. 13 Capillaries form Microcirculation Microscopic vessels that connect arterioles to venules
Found near every cell in the body but more extensive in highly active tissue (muscles, liver, kidneys & brain)
entire capillary bed fills with blood when tissue is active
lacking in epithelia, cornea and lens of eye & cartilage
Function is exchange of nutrients & wastes between blood and tissue fluid
Capillary walls are composed of only a single layer of cells (endothelium) and a basement membrane.
14. 14 Types of Capillaries Continuous capillaries
intercellular clefts are gaps between neighboring cells
skeletal & smooth, connective tissue and lungs
Fenestrated capillaries
plasma membranes have many holes
kidneys, small intestine, choroid plexuses, ciliary process & endocrine glands
Sinusoids
very large fenestrations
incomplete basement membrane
liver, bone marrow, spleen, anterior pituitary, & parathyroid gland
15. 15 Venules Small veins collecting blood from capillaries
Tunica media contains only a few smooth muscle cells & scattered fibroblasts
very porous endothelium allows for escape of many phagocytic white blood cells
Venules that approach size of veins more closely resemble structure of vein
16. 16 Veins Veins consist of the same three tunics as arteries but have a thinner tunica interna and media and a thicker tunica externa
less elastic tissue and smooth muscle
thinner-walled than arteries
contain valves to prevent the backflow of blood.
Vascular (venous) sinuses are veins with very thin walls with no smooth muscle to alter their diameters. Examples are the brain�s superior sagittal sinus and the coronary sinus of the heart.
17. 17 Veins Proportionally thinner walls than same diameter artery
tunica media less muscle
lack external & internalelastic lamina
Still adaptable to variationsin volume & pressure
Valves are thin folds of tunica interna designed to prevent backflow
18. 18 Varicose Veins Twisted, dilated superficial veins
caused by leaky venous valves
congenital or mechanically stressed from prolonged standing or pregnancy
allow backflow and pooling of blood
extra pressure forces fluids into surrounding tissues
nearby tissue is inflamed and tender
The most common sites for varicose veins are in the esophagus, superficial veins of the lower limbs, and veins in the anal canal (hemorrhoids). Deeper veins not susceptible because of support of surrounding muscles
The treatments for varicose veins in the lower limbs include: sclerotherapy, radiofrequency endovenous occlusion, laser occlusion, and surgical stripping
19. 19 Blood Distribution 60% of blood volume at rest is in systemic veins and venules
function as blood reservoir
veins of skin & abdominalorgans (liver and spleen)
blood is diverted from it intimes of need
increased muscular activityproduces venoconstriction
hemorrhage causes
venoconstriction to help
maintain blood pressure
15% of blood volume in arteries & arterioles
20. 20 Anastomoses Union of 2 or more arteries supplying the same body region
blockage of only one pathway has no effect
circle of willis underneath brain
coronary circulation of heart
Alternate route of blood flow through an anastomosis is known as collateral circulation
can occur in veins and venules as well
Arteries that do not anastomose are known as end arteries. Occlusion of an end artery interrupts the blood supply to a whole segment of an organ, producing necrosis (death) of that segment.
Alternate routes to a region can also be supplied by nonanastomosing vessels.
21. 21 Capillary Exchange Movement of materials in & out of a capillary
diffusion (most important method)
Substances such as O2, CO2, glucose, amino acids, hormones, and others diffuse down their concentration gradients.
all plasma solutes except large proteins pass freely across
through lipid bilayer, fenestrations or intercellular clefts
blood brain barrier does not allow diffusion of water-soluble materials (nonfenestrated epithelium with tight junctions)
transcytosis
passage of material across endothelium in tiny vesicles by endocytosis and exocytosis
large, lipid-insoluble molecules such as insulin or maternal antibodies passing through placental circulation to fetus
bulk flow (see next slide)
22. 22 Bulk Flow: Filtration & Reabsorption Movement of large amount of dissolved or suspended material in same direction
move in response to pressure
from area of high pressure to area of low
faster rate of movement than diffusion or osmosis
Most important for regulation of relative volumes of blood & interstitial fluid
filtration is movement of material into interstitial fluid
promoted by blood hydrostatic pressure & interstitial fluid osmotic pressure
reabsorption is movement from interstitial fluid into capillaries
promoted by blood colloid osmotic pressure
balance of these pressures is net filtration pressure
23. 23 Starling�s law of the capillaries is that the volume of fluid & solutes reabsorbed is almost as large as the volume filtered.
24. 24 Net Filtration Pressure Whether fluids leave or enter capillaries depends on net balance of pressures
net outward pressure of 10 mm Hg at arterial end of a capillary bed
net inward pressure of 9 mm Hg at venous end of a capillary bed
About 85% of the filtered fluid is returned to the capillary
escaping fluid and plasma proteins are collected by lymphatic capillaries (3 liters/day)
25. 25 Edema An abnormal increase in interstitial fluid if filtration exceeds reabsorption
result of excess filtration
increased blood pressure (hypertension)
increased permeability of capillaries allows plasma proteins to escape
result of inadequate reabsorption
decreased concentration of plasma proteins lowers blood colloid osmotic pressure
inadequate synthesis or loss from liver disease, burns, malnutrition or kidney disease blockage of lymphatic vessels postoperatively or due to filarial worm infection
Often not noticeable until 30% above normal
26. 26 HEMODAYNAMICS: FACTORS AFFECTING BLOOD FLOW The distribution of cardiac output to various tissues depends on the interplay of the pressure difference that drives the blood flow and the resistance to blood flow.
Blood pressure (BP) is the pressure exerted on the walls of a blood vessel; in clinical use, BP refers to pressure in arteries.
Cardiac output (CO) equals mean aortic blood pressure (MABP) divided by total resistance (R).
27. 27 Hemodynamics - Overview Factors that affect blood pressure include cardiac output, blood volume, viscosity, resistance, and elasticity of arteries.
As blood leaves the aorta and flows through systemic circulation, its pressure progressively falls to 0 mm Hg by the time it reaches the right atrium.
Resistance refers to the opposition to blood flow as a result of friction between blood and the walls of the blood vessels.
Vascular resistance depends on the diameter of the blood vessel, blood viscosity, and total blood vessel length.
Systemic vascular resistance (also known as total peripheral resistance) refers to all of the vascular resistances offered by systemic blood vessels; most resistance is in arterioles, capillaries, and venules due to their small diameters.
28. 28 Hemodynamics Factors affecting circulation
pressure differences that drive the blood flow
velocity of blood flow
volume of blood flow
blood pressure
resistance to flow
venous return
An interplay of forces result in blood flow
29. 29 Volume of Blood Flow Cardiac output = stroke volume x heart rate
Other factors that influence cardiac output
blood pressure
resistance due to friction between blood cells and blood vessel walls
blood flows from areas of higher pressure to areas of lower pressure
30. 30 Blood Pressure Pressure exerted by blood on walls of a vessel
caused by contraction of the ventricles
highest in aorta
120 mm Hg during systole & 80during diastole
If heart rate increases cardiac output, BP rises
Pressure falls steadily in systemic circulation with distance from left ventricle
35 mm Hg entering the capillaries
0 mm Hg entering the right atrium
If decrease in blood volume is over 10%, BP drops
Water retention increases blood pressure
31. 31 Velocity of Blood Flow The volume that flows through any tissue in a given period of time is blood flow.
The velocity of blood flow is inversely related to the cross-sectional area of blood vessels; blood flows most slowly where cross-sectional area is greatest.
Blood flow decreases from the aorta to arteries to capillaries and increases as it returns to the heart.
32. 32 Velocity of Blood Flow Speed of blood flow in cm/sec is
inversely related to cross-sectional area
blood flow is slower in thearterial branches
flow in aorta is 40 cm/sec whileflow in capillaries is .1 cm/sec
slow rate in capillaries allows forexchange
Blood flow becomes faster when vessels merge to form veins
Circulation time is time it takes a drop of blood to travel from right atrium back to right atrium
33. 33 Venous Return Volume of blood flowing back to the heart from the systemic veins
depends on pressure difference
from venules (16 mm Hg) to right
atrium (0 mm Hg)
tricuspid valve leaky and buildup
of blood on venous side of circulation
Skeletal muscle pump
contraction of muscles & presence of valves
Respiratory pump
decreased thoracic pressure and increased abdominal pressure during inhalation, moves blood into thoracic veins and the right atrium
34. 34 Clinical Application Syncope, or fainting, refers to a sudden, temporary loss of consciousness followed by spontaneous recovery. It is most commonly due to cerebral ischemia but it may occur for several other reasons
35. 35 Factors that Increase Blood Pressure
36. 36 Resistance Friction between blood and the walls of vessels
average blood vessel radius
smaller vessels offer more resistance to blood flow
cause moment to moment fluctuations in pressure
blood viscosity (thickness)
ratio of red blood cells to plasma volume
increases in viscosity increase resistance
dehydration or polycythemia
total blood vessel length
the longer the vessel, the greater the resistance to flow
200 miles of blood vessels for every pound of fat
obesity causes high blood pressure
Systemic vascular resistance is the total of above
arterioles control BP by changing diameter
37. 37 Control of Blood Pressure & Flow Role of cardiovascular center
help regulate heart rate & stroke volume
specific neurons regulate blood vessel diameter
38. 38 Cardiovascular Center - Overview The cardiovascular center (CV) is a group of neurons in the medulla that regulates heart rate, contractility, and blood vessel diameter.
input from higher brain regions and sensory receptors (baroreceptors and chemoreceptors)
output from the CV flows along sympathetic and parasympathetic fibers.
Sympathetic impulses along cardioaccelerator nerves increase heart rate and contractility.
Parasympathetic impulses along vagus nerves decrease heart rate.
The sympathetic division also continually sends impulses to smooth muscle in blood vessel walls via vasomotor nerves. The result is a moderate state of tonic contraction or vasoconstriction, called vasomotor tone.
39. 39 Input to the Cardiovascular Center Higher brain centers such as cerebral cortex, limbic system & hypothalamus
anticipation of competition
increase in body temperature
Proprioceptors
input during physical activity
Baroreceptors
changes in pressure within blood vessels
Chemoreceptors
monitor concentration of chemicals in the blood
40. 40 Output from the Cardiovascular Center Heart
parasympathetic (vagus nerve)
decrease heart rate
sympathetic (cardiac accelerator nerves)
cause increase or decrease in contractility & rate
Blood vessels
sympathetic vasomotor nerves
continual stimulation to arterioles in skin & abdominal viscera producing vasoconstriction (vasomotor tone)
increased stimulation produces constriction & increased BP
41. 41 Neural Regulation of Blood Pressure Baroreceptors are important pressure-sensitive sensory neurons that monitor stretching of the walls of blood vessels and the atria.
The cardiac sinus reflex is concerned with maintaining normal blood pressure in the brain and is initiated by baroreceptors in the wall of the carotid sinus.
The aortic reflex is concerned with general systemic blood pressure and is initiated by baroreceptors in the wall of the arch of the aorta or attached to the arch.
If blood pressure falls, the baroreceptor reflexes accelerate heart rate, increase force of contraction, and promote vasoconstriction.
42. 42 Neural Regulation of Blood Pressure Baroreceptor reflexes
carotid sinus reflex
swellings in internal carotid artery wall
glossopharyngeal nerve to cardiovascular center in medulla
maintains normal BP in the brain
aortic reflex
receptors in wall of ascending aorta
vagus nerve to cardiovascular center
maintains general systemic BP
If feedback is decreased, CV center reduces parasympathetic & increases sympathetic stimulation of the heart
43. 43 Innervation of the Heart Speed up the heart with sympathetic stimulation
Slow it down with parasympathetic stimulation (X)
Sensory information from baroreceptors (IX)
44. 44 Carotid Sinus Massage & Syncope Carotid sinus massage can slow heart rate in paroxysmal superventricular tachycardia
Stimulation (careful neck massage) over the carotid sinus lowers heart rate
paroxysmal superventricular tachycardia
tachycardia originating from the atria
Anything that puts pressure on carotid sinus
tight collar or hyperextension of the neck
may slow heart rate & cause carotid sinus syncope or fainting
45. 45 Syncope Fainting or a sudden, temporary loss of consciousness not due to trauma
due to cerebral ischemia or lack of blood flow to the brain
Causes
vasodepressor syncope = sudden emotional stress
situational syncope = pressure stress of coughing, defecation, or urination
drug-induced syncope = antihypertensives, diuretics, vasodilators and tranquilizers
orthostatic hypotension = decrease in BP upon standing
46. 46 Chemoreceptor Reflexes Carotid bodies and aortic bodies
detect changes in blood levels of O2, CO2, and H+ (hypoxia, hypercapnia or acidosis )
causes stimulation of cardiovascular center
increases sympathetic stimulation to arterioles & veins
vasoconstriction and increase in blood pressure
Also changes breathing rates as well
47. 47 Hormonal Regulation of Blood Pressure Renin-angiotensin-aldosterone system
decrease in BP or decreased blood flow to kidney
release of renin / results in formation angiotensin II
systemic vasoconstriction
causes release aldosterone (H2O & Na+ reabsorption)
Epinephrine & norepinephrine
increases heart rate & force of contraction
causes vasoconstriction in skin & abdominal organs
vasodilation in cardiac & skeletal muscle
ADH causes vasoconstriction
ANP (atrial natriuretic peptide) lowers BP
causes vasodilation & loss of salt and water in the urine
48. 48 Local Regulation of Blood Pressure The ability of a tissue to automatically adjust its own blood flow to match its metabolic demand for supply of O2 and nutrients and removal of wastes is called autoregulation.
Local factors cause changes in each capillary bed
important for tissues that have major increases in activity (brain, cardiac & skeletal muscle)
Local changes in response to physical changes
warming & decrease in vascular stretching promotes vasodilation
Vasoactive substances released from cells alter vessel diameter (K+, H+, lactic acid, nitric oxide)
systemic vessels dilate in response to low levels of O2
pulmonary vessels constrict in response to low levels of O2
49. 49 Evaluating Circulation Pulse is a pressure wave
alternate expansion & recoil of elastic artery after each systole of the left ventricle
pulse rate is normally between 70-80 beats/min
tachycardia is rate over 100 beats/min/bradycardia under 60
Measuring blood pressure with sphygmomanometer
Korotkoff sounds are heard while taking pressure
systolic blood pressure is recorded during ventricular contraction
diastolic blood pressure is recorded during ventricular contraction
provides information about systemic vascular resistance
pulse pressure is difference between systolic & diastolic
normal ratio is 3:2:1 -- systolic/diastolic/pulse pressure
50. 50 Pulse Points
51. 51 Evaluating Circulation
52. 52 Blood Pressure The normal blood pressure of a young adult male is 120/80 mm Hg (8-10 mm Hg less in a young adult female). The range of average values varies with many factors.
Pulse pressure is the difference between systolic and diastolic pressure. It normally is about 40 mm Hg and provides information about the condition of the arteries.
53. 53 SHOCK AND HOMEOSTASIS Shock is an inadequate cardiac output that results in failure of the cardiovascular system to deliver adequate amounts of oxygen and nutrients to meet the metabolic needs of body cells. As a result, cellular membranes dysfunction, cellular metabolism is abnormal, and cellular death may eventually occur without proper treatment.
inadequate perfusion
cells forced to switch to anaerobic respiration
lactic acid builds up
cells and tissues become damaged & die
54. 54 Types of Shock Hypovolemic shock is due to decreased blood volume.
Cardiogenic shock is due to poor heart function.
Vascular shock is due to inappropriate vasodilation.
Obstructive shock is due to obstruction of blood flow.
Homeostatic responses to shock include activation of the renin-angiotensin-aldosterone system, secretion of ADH, activation of the sympathetic division of the ANS, and release of local vasodilators.
Signs and symptoms of shock include clammy, cool, pale skin; tachycardia; weak, rapid pulse; sweating; hypotension (systemic pressure < 90 mm HG); altered mental status; decreased urinary output; thirst; and acidosis.
55. 55 Types of Shock Hypovolemic shock due to loss of blood or body fluids (hemorrhage, sweating, diarrhea)
venous return to heart declines & output decreases
Cardiogenic shock caused by damage to pumping action of the heart (MI, ischemia, valve problems or arrhythmias)
Vascular shock causing drop inappropriate vasodilation -- anaphylatic shock, septic shock or neurogenic shock (head trauma)
Obstructive shock caused by blockage of circulation (pulmonary embolism)
56. 56 Homeostatic Responses to Shock Mechanisms of compensation in shock attempt to return cardiac output & BP to normal
activation of renin-angiotensin-aldosterone
secretion of antidiuretic hormone
activation of sympathetic nervous system
release of local vasodilators
If blood volume drops by 10-20% or if BP does not rise sufficiently, perfusion may be inadequate -- cells start to die.
57. 57 Restoring BP during Hypovolemic Shock
58. 58 Signs & Symptoms of Shock Rapid resting heart rate (sympathetic stimulation)
Weak, rapid pulse due to reduced cardiac output & fast heart rate
Clammy, cool skin due to cutaneous vasoconstriction
Sweating -- sympathetic stimulation
Altered mental state due to cerebral ischemia
Reduced urine formation -- vasoconstriction to kidneys & increased aldosterone & antidiuretic hormone
Thirst -- loss of extracellular fluid
Acidosis -- buildup of lactic acid
Nausea -- impaired circulation to GI tract
59. 59 Introduction The blood vessels are organized into routes that deliver blood throughout the body.
The largest circulatory route is the systemic circulation.
Other routes include pulmonary circulation and fetal circulation.
60. 60 Circulatory Routes Systemic circulation is left side heart to body & back to heart
Hepatic Portal circulation is capillaries of GI tract to capillaries in liver
Pulmonary circulation is right-side heart to lungs & back to heart
Fetal circulation is from fetal heart through umbilical cord to placenta & back
61. 61 Systemic Circulation The systemic circulation takes oxygenated blood from the left ventricle through the aorta to all parts of the body, including some lung tissue (but does not supply the air sacs of the lungs) and returns the deoxygenated blood to the right atrium.
The aorta is divided into the ascending aorta, arch of the aorta, and the descending aorta.
Each section gives off arteries that branch to supply the whole body.
Blood returns to the heart through the systemic veins. All the veins of the systemic circulation flow into the superior or inferior vena cavae or the coronary sinus, which in turn empty into the right atrium.
62. 62 Arterial Branches of Systemic Circulation All are branches from aorta supplying arms, head, lower limbs and all viscera with O2 from the lungs
Aorta arises from left ventricle (thickest chamber)
4 major divisions of aorta
ascending aorta
arch of aorta
thoracic aorta
abdominal aorta
63. 63 Aorta and Its Superior Branches Aorta is largest artery of the body
ascending aorta
2 coronary arteries supply myocardium
arch of aorta -- branches to the arms & head
brachiocephalic trunk branches into right common carotid and right subclavian
left subclavian & left carotid arise independently
thoracic aorta supplies branches to pericardium, esophagus, bronchi, diaphragm, intercostal & chest muscles, mammary gland, skin, vertebrae and spinal cord
64. 64 Coronary Circulation Right & left coronary arteries branch to supply heart muscle
anterior & posterior interventricular aa.
65. 65 Subclavian Branches Subclavian aa. pass superior to the 1st rib
gives rise to vertebral a. that supplies blood to the Circle of Willis on the base of the brain
Become the axillary artery in the armpit
Become the brachial in the arm
Divide into radial and ulnar branches in the forearm
66. 66 Common Carotid Branches External carotid arteries
supplies structures external to skull as branches of maxillary and superficial temporal branches
Internal carotid arteries (contribute to Circle of Willis)
supply eyeballs and parts of brain
67. 67 Abdominal Aorta and Its Branches Supplies abdominal & pelvic viscera & lower extremities
celiac aa. supplies liver, stomach, spleen & pancreas
superior & inferior mesenteric aa. supply intestines
renal aa supply kidneys
gonadal aa. supply ovariesand testes
Splits into common iliacaa at 4th lumbar vertebrae
external iliac aa supplylower extremity
internal iliac aa supplypelvic viscera
68. 68 Visceral Branches off Abdominal Aorta Celiac artery is first branch inferior to diaphragm
left gastric artery, splenic artery, common hepatic artery
Superior mesenteric artery lies in mesentery
pancreaticoduodenal, jejunal, ileocolic, ascending & middle colic aa.
Inferior mesenteric artery
descending colon, sigmoid colon & rectal aa
69. 69 Arteries of the Lower Extremity External iliac artery become femoral artery when it passes under the inguinal ligament & into the thigh
femoral artery becomes popliteal artery behind the knee
70. 70 Veins of the Systemic Circulation Drain blood from entire body & return it to right side of heart
Deep veins parallel the arteries in the region
Superficial veins are found just beneath the skin
All venous blood drains to either superior or inferior vena cava or coronary sinus
71. 71 Major Systemic Veins All empty into the right atrium of the heart
superior vena cava drains the head and upper extremities
inferior vena cava drains the abdomen, pelvis & lower limbs
coronary sinus is large vein draining the heart muscle back into the heart
72. 72 Veins of the Head and Neck External and Internal jugular veins drain the head and neck into the superior vena cava
Dural venous sinuses empty into internal jugular vein
73. 73 Venipuncture Venipuncture is normally performed at cubital fossa, dorsum of the hand or great saphenous vein in infants.
74. 74 Hepatic Portal Circulation A portal system carries blood between two capillary networks, in this case from capillaries of the gastrointestinal tract to sinusoids of the liver.
The hepatic portal circulation collects blood from the veins of the pancreas, spleen, stomach, intestines, and gallbladder and directs it into the hepatic portal vein of the liver before it returns to the heart.
It enables nutrient utilization and blood detoxification by the liver.
75. 75 Hepatic Portal System Subdivision of systemic circulation
Detours venous blood from GI tract to liver on its way to the heart
liver stores or modifies nutrients
Formed by union of splenic, superior mesenteric & hepatic veins
76. 76 Arterial Supply and Venous Drainage of Liver
77. 77 Pulmonary Circulation The pulmonary circulation takes deoxygenated blood from the right ventricle to the air sacs of the lungs and returns oxygenated blood from the lungs to the left atrium.
The pulmonary and systemic circulations differ from each other in several more ways.
Blood in the pulmonary circulation is not pumped so far as in the systemic circulation and the pulmonary arteries have a larger diameter, thinner walls, and less elastic tissue.
resistance to blood flow is very low meaning that less pressure is needed to move blood through the lungs.
normal pulmonary capillary hydrostatic pressure is lower than systemic capillary hydrostatic pressure which tends to prevent pulmonary edema.
78. 78 Pulmonary Circulation
79. 79 Pulmonary Circulation Carries deoxygenated blood from right ventricle to air sacs in the lungs and returns it to the left atria
Vessels include pulmonary trunk, arteries and veins
Differences from systemic circulation
pulmonary aa. are larger, thinner with less elastic tissue
resistance to is low & pulmonary blood pressure is reduced
80. 80 Fetal Circulation Oxygen from placenta reaches heart via fetal veins in umbilical cord.
bypasses liver
Heart pumps oxygenated blood to capillaries in all fetal tissues including lungs.
Umbilical aa. Branch off iliac aa. to return blood to placenta.
81. 81 Lung Bypasses in Fetal Circulation
82. 82 DEVELOPMENT OF BLOOD VESSELS AND BLOOD Development of blood cells and blood vessels begins at 15 � 16 days.
It begins in the mesoderm of the yolk sac, chorion, and body stalk.
A few days later vessels begin to form within the embryo
Blood vessels and blood cells develop from hemangioblasts.
83. 83 Aging and the Cardiovascular System General changes associated with aging
decreased compliance of aorta
reduction in cardiac muscle fiber size
reduced cardiac output & maximum heart rate
increase in systolic pressure
Total cholesterol & LDL increases, HDL decreases
Congestive heart failure, coronary artery disease and atherosclerosis more likely
84. 84 DISORDERS: HOMEOSTATIC IMBALANCES Hypertension, or persistently high blood pressure, is defined as systolic blood pressure of 140 mm Hg or greater and diastolic blood pressure of 90 mm Hg or greater.
Primary hypertension (approximately 90-95% of all hypertension cases) is a persistently elevated blood pressure that cannot be attributed to any particular organic cause.
Secondary hypertension (the remaining 5-10% of cases) has an identifiable underlying cause such as obstruction of renal blood flow or disorders that damage renal tissue, hypersecretion of aldosterone, or hypersecretion of epinephrine and norepinephrine by pheochromocytoma, a tumor of the adrenal gland.
85. 85 DISORDERS: HOMEOSTATIC IMBALANCES High blood pressure can cause considerable damage to the blood vessels, heart, brain, and kidneys before it causes pain or other noticeable symptoms.
Lifestyle changes that can reduce elevated blood pressure include losing weight, limiting alcohol intake, exercising, reducing sodium intake, maintaining recommended dietary intake of potassium, calcium, and magnesium, not smoking, and managing stress.
Various drugs including diuretics, beta blockers, vasodilators, and calcium channel blockers have been used to successfully treat hypertension.