ARTIFICIAL SKIN
ARTIFICIAL SKIN. PRESENTED BY. PWADUBASAHIYI COSTON PWAVODI 20143883 MSC. FELIX CHIBUZO OBI 20144610 MSC. MICHAEL OLABOYE AMUSAN 20103181 ARTIFICIAL ORGANS DEPARTMENT OF BIOMEDICAL ENGINEERING. INTRODUCTION.

ARTIFICIAL SKIN
E N D
Presentation Transcript
ARTIFICIAL SKIN PRESENTED BY PWADUBASAHIYI COSTON PWAVODI 20143883 MSC. FELIX CHIBUZO OBI 20144610 MSC. MICHAEL OLABOYE AMUSAN 20103181 ARTIFICIAL ORGANS DEPARTMENT OF BIOMEDICAL ENGINEERING..
INTRODUCTION • The term artificial skin is used to describe any material used to replace (permanently or temporarily) or to mimic the dermal and epidermal layers of the skin. • The primary current application of artificial skin is for the treatment of skin loss or damage on burn patients. • Alternatively however, artificial skin is now being used in some places to treat patients with skin diseases, such as diabetic foot ulcers, and severe .[1]
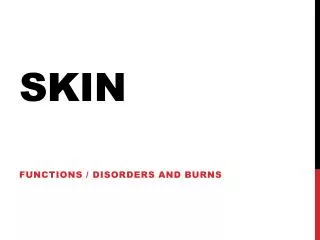
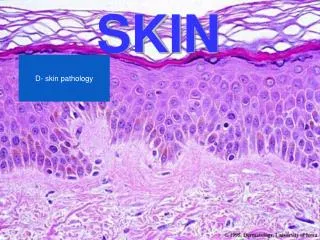
ANATOMICAL OVERVIEW OF THE SKIN • Human skin is comprised of two primary layers, the dermis and the epidermis. A diagram of a typical section of human skin is shown here. The epidermis is comprised of keratinocytes of varying levels of differentiation. • As can be seen in the figure, the epidermis contains no blood vessels meaning transport of nutrients to the epidermis occurs from the dermis below [2].
BRIEF HISTORY OF THE ARTIFICIAL SKIN • 3000-2500BC, India: Skin is allegedly transplanted by Hindus from the buttocks to repair mutilated ears and noses. • 1442, Italy: An allogenous skin graft was performed by Branca de Branca who used a man’s arm skin to transplant the nose of the man’s slave onto himself. • 1871, England: Pollock proposes skin grafts for burn treatment. • 1998, United States: First tissue engineered skin (Apligraf) is approved by the FDA. • 2001, United States: Dermagraft, Orcel, Composite Cultured Skin are FDA approved [4]. • 2002, United States: Integra is FDA approved for treatment of severe burns [4].
PROCESSES INVOLVED IN THE MANUFACTURE OF THE ARTIFICIAL SKIN Skin is usually donated by other donors. • Fibroblasts are removed from the donated skin and are frozen until they are needed. • The fibroblasts are placed on a polymeric mesh scaffolding, gather oxygen, and grow new cells. • The cells are then transferred to a culture system.After 4 weeks the polymer mesh dissolves and leaves behind a new layer of dermal skin. • When the growth cycle is completed, they add more nutrients. Keratinocytes are added to the collagen and are exposed to air to form epidermal layers. • The skin is now completed and is stored in sterile contains until ready to use.
Skin Grafts • Skin grafts are required for patients with skin damage that is too significant for self-repair. As stated before, one of the primary requirements for artificial skin is for the treatment of severe burn victims. [2 • Skin grafts are also often done on patients with ulcers, skin loss from cancer removal, and plastic surgery [1] • The skin required for a skin graft can be obtained from three sources; the patient themselves (autograft), another human (allograft), or from animals such as pigs or cows (xenografts)[2]. Allografts and xenografts can only be used as temporary wound coverings as they are typically rejected within 7 to 10 days or 3 to 5 days respectively [2].
Artificial Skin Treatments • Since 2001, a total of 4 skin repair devices have been FDA approved. These include Dermagraf, Orcel, Integra, and Composite Cultured Skin [4]. Composite Cultured Skin is specifically for children with recessive dystrophic epidermolysisbullosa and also contain living cells.
AREAS OF APPLICATION Artificial Skins are primarily used for the Treatment of Skin loss or damage on burn Patients. Alternative Areas of Application of Artificial Skins includes • -Treatment of patients with skin diseases, such as diabetic foot ulcers, and severe scarring. • - Plastics and Cosmetic Surgery.
ADVANTAGES AND DISADVANTAGES ADVANTAGES • -Chances of survival for burn patients. • -Artificial skin seals the wound preventing fluid loss and bacteria from entering through the wound. • - The fear of Stigmatization of the Patient is eliminated DISADVANTAGES • -Risks of Infection and Rejection by the Patients • -Lack of vascularization to the implanted skin or skin cells can lead to cell death which provides a breeding ground for bacteria. • -Loss of Sensitivity • -Cut of Blood Supply. • -Complication could arise due to Skin Adhesion and/or fluid buildup between the wounded site and the transplanted skin. • - Artificial Skins are very expensive.
Interesting, right? This is just a sneak preview of the full presentation. We hope you like it! To see the rest of it, just click here to view it in full on PowerShow.com. Then, if you’d like, you can also log in to PowerShow.com to download the entire presentation for free.