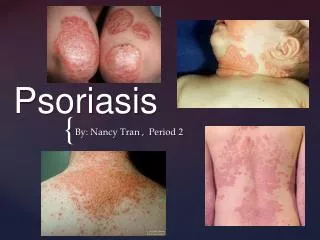
Psoriasis
* For Best Viewing: Open in Slide Show Mode Click on icon or From the View menu, select the Slide Show option. * To help you as you prepare a talk, we have included the relevant text from ITC in the notes pages of each slide . Psoriasis. What are the most common symptoms?.

Psoriasis
E N D
Presentation Transcript
* For Best Viewing: Open in Slide Show Mode Click on icon orFrom the View menu, select the Slide Show option * To help you as you prepare a talk, we have included the relevant text from ITC in the notes pages of each slide
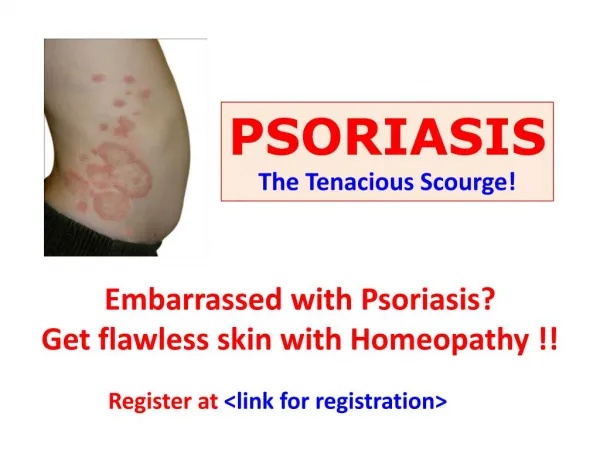
What are the most common symptoms? • Erythematous lesions with loose, silvery-white scales • Removing scale can induce punctate bleeding: Auspitz sign • Papules can coalesce in pruritic patches / plaques • Nails and joints may be affected A. Extensive, well-demarcated erythematous plaques of abdomen
B. Erythematous plaque of elbow C. Erythematous, scaling plaques of abdomen
What is the differential diagnosis? • Plaque • Eczema; dermatophyte infection; superficial squamous / basal cell CA; subacutecutaneous lupus • Guttate • Secondary syphilis; pityriasisrosea • Erythrodermic • Pityriasisrubrapilaris; drug eruptions • Pustular • Candidiasis; acute generalized exanthematicpustulosis • Inverse • Intertrigo; cutaneous T-cell lymphoma
Which areas of the skin are most commonly affected? • In chronic plaque psoriasis • Extensor surfaces (elbows and knees) • Lumbosacral area • Intergluteal cleft • Scalp • In inverse psoriasis • Intertriginous areas
How often are the nails involved? • Up to 55% with psoriasis have nail involvement • Occurs in any subtype • <5% of nail disease occurs in those lacking other cutaneous findings of psoriasis • ≤90% with psoriatic arthritis have nail involvement • Fingernail involvement in 50% of cases • Toenail involvement in 30% of cases • Requires aggressive treatment: intralesional steroid injections
How often are joints affected by psoriasis? Which ones? • Psoriatic arthritis occurs in up to 30% • Inflammatory, seronegativespondyloarthropathy • Stiffness, pain, swelling of joints, ligaments, tendons • Hands more likely involved than feet • Polyarticular peripheral joint involvement common • About 5% have only axial involvement • Up to 50% have both spine & peripheral joint involvement
Enthesitis: inflammation where tendon, ligament, or joint capsule fibers insert into bone • Dactylitis: enthesitis of tendons and ligaments + synovitis of an entire digit
When should joints be tapped to diagnose PsA? • Use clinical observations • Symmetrical joint stiffness (hands, feet, large joints) for ≥30 minutes in morning or after long periods of inactivity • Use radiologic observations • Joint erosions, joint-space narrowing • Bony proliferation, spur formation • Osteolysis with “pencil-in-cup” deformities • Arthrocentesis is not recommended
Aside from skin and joints, what else should be examined when considering a diagnosis of psoriasis? • Psoriasis: systemic inflammatory disorder • Inflammation cascade promotes endothelial dysfunction and oxidative stress • Increases risk for: • Atherosclerosis-based CV disease • Hypertension • Obesity and the metabolic syndrome • Diabetes • Smoking
What triggers or unmasks psoriasis? • Bacterial and viral infections • URI associated with guttate psoriasis • Especially Streptococcus pyogenes • Stress • Often first outbreak traced to stressful event • Lesions can be induced locally in areas of physical trauma, i.e., vaccination, tattoos, sunburn, excoriation • Certain medications • Lithium, interferon, antimalarials, β-blockers, ACE inhibitors, NSAIDs, withdrawal of oral corticosteroids • Cold weather with low humidity
Are there any specific diagnostic tests for psoriasis? • No • Diagnosis is clinical • For initial work-up: • Total body skin evaluation, including nails and scalp • ? Joint symptoms (stiffness, swelling, pain, decreased ROM) • ? Personal or family history of autoimmune diseases
Which blood tests are abnormal in psoriasis, and how specific are they to the diagnosis? • Rarely needed for diagnosis • Rapid plasma reagin: to distinguish from syphilis • Antinuclear antibody, anti-Ro, and anti-La: confirms Dx if subacutecutaneous lupus suspected • CRP levels: occasionally elevated in PsA • Uric acid levels: may be elevated, especially inerythrodermic psoriasis
What is the role of skin biopsy in making the diagnosis? • Histologic confirmation • Classic findings of psoriasis • Epidermal hyperplasia • Parakeratosis • Thinning of granular layer • Neutrophil + lymphocyte infiltration in epidermis and dermis • Increased prominence of dermal papillary vasculature
CLINICAL BOTTOM LINE: Diagnosis and Evaluation… • Diagnosis most often made clinically • Psoriasis papules, patches, or plaques: sharply demarcated, erythematous, scaly, pruritic • Concomitant joint and nail involvement • Histologic and lab abnormalities not required • Triggers: infection, trauma, stress, and certain drugs • Psoriasis increases risk for CV disease and events • If diagnosis uncertain, consult dermatologist
What drug therapies are used in treatment? • Topical therapies • Corticosteroids • Vitamin D analogues • Topical retinoids • Calcineurin inhibitors • Salicylic acid • Anthralin • Coal tar • Phototherapy • Systemic therapies • Methotrexate • Cyclosporine A • Oral vitamin A derivatives • Biological therapies • Adalimumab • Alefacept • Etanercept • Golimumab • Infliximab • Ustekinumab
How should a clinician choose between topical and systemic drug therapy? • Determine disease severity • Measure affected body surface area • ≤3%: mild • 3%-10%: moderate • ≥10% or serious adverse affect on QOL: severe • Determine the location of lesions • Consider affect on QOL • Mild disease: topical therapies • Moderate-to-severe disease: systemic and topical therapies; biologics if systemics fail / can’t be used
What is the role of phototherapy? • For widespread disease or when disease substantially affects QOL • Efficacious and cost-effective • Not immunosuppressive like systemic drugs • Affects Langerhans cells directly, cytokines indirectly • Don’t use with photosensitive disorders
Is there a role for combination drug therapy and phototherapy? • Improves efficacy and decreases toxicity of a potentially hazardous combination agent Phototherapy can be combined with: • Anthralin or coal tar • MTX • Retinoids • Biological therapies
What alternative therapies are shown to improve quality of life and outcomes? • Salicylic acid • Combine with other topical therapies • Dead Sea • Unique UVA-UVB ratio + high water salinity improves psoriasis • May increase risk for nonmelanoma skin cancer
How should psoriasis be treated in pregnant patients? • Consider therapy benefits vs. potential fetal risk • First-line treatment: topical agent or phototherapy • Alternative to phototherapy: TNF-α blocker (Category B) • Severe psoriasis: cyclosporine A (Category C) • Contraindicated: retinoids, MTX, oral vitamin A derivatives
When is it necessary to hospitalize patients with psoriasis? • Erythrodermic psoriasis • Inflammation of ≥75% BSA +/- presence of exfoliation • Triggers: steroid withdrawal, sun exposure, drug reactions, emotional stress • First-line: adjuvant topical treatment + CSA or infliximab • Hospitalize for hypothermia or hyperthermia, protein loss, dehydration, infection, renal failure, hi-output cardiac failure • Acute episodes of generalized pustular psoriasis • Pinhead-sized pustules on erythematous background • Pustules may dry out, exfoliate, and redevelop • Triggers: corticosteroid withdrawal for plaque psoriasis • Retinoids uniquely effective treatment • Hospitalize for systemic symptoms
When should patients be referred to a dermatologist? • Recalcitrant disease • Moderate-to-severe disease • Disease that significantly impairs quality of life • Dermatologist can initiate • Phototherapy • Systemic therapy • Combination therapy
When should patients be referred to a rheumatologist? • When PsA is diagnosed • Majority have psoriasis years before joint symptoms develop • Rheumatologist guides treatment to • Alleviate pain and swelling • Inhibit structural damage • Improve quality of life
When should patients be referred to a psychiatrist? Order a consultation if psychiatric disorder suspected • Screen for psychosocial aspects • Psychosocial morbidity + decreased occupational function • Clinical severity may not reflect extent of emotional impact
What is the role of the PCP in treating psoriasis? • Identify conditions associated with psoriasis • Help prevent comorbid conditions • Provide counsel regarding lifestyle modifications • Consult specialists (dermatology, rheumatology)
How often should patients be followed by a dermatologist? • Regularly to assess: • Disease severity • Compliance and medication toxicity • Quality-of-life issues • Topical steroids: every 6-12 months • More frequently if using more potent topical steroids • Systemics: Follow more frequently • MTX/CsA: Examine for response and skin cancer • Phototherapy: annually • Check for photoaging, pigmentation, skin cancer
Should patients be routinely followed by other specialists? • Mild PsA: PCP • Treat with NSAIDs or intra-articular steroid injections • Moderate-to-severe PsA: rheumatologist / dermatologist • Risk for structural damage • More aggressive therapy required
CLINICAL BOTTOM LINE: Treatment and management… • Mild-to-moderate psoriasis • Topical therapy: steroid, vitamin D analogue, retinoid, calcineurin inhibitor • Moderate-to-severe psoriasis • Traditional systemic medications, biological agents, or phototherapy + topical therapy • For PsA, start treatment early to avoid structural damage • Mild disease: NSAIDs • More severe systemic disease: biological agent, MTX, or a combination of the two
How should patients be educated about psoriasis pathophysiology and genetics? • Normal skin cells: mature + fall off body in 28 days • Psoriasis skin cells: mature in just 3 to 4 days + pile up into lesions instead of shedding • Requires both inheritance + environmental trigger • ≥10% of general population inherits ≥1 predisposing gene • But only 3% of population develops psoriasis • If both parents have psoriasis, offspring incidence up to 50% • If 1 parent affected, offspring incidence 16% • If only a sibling affected, incidence 8%
What should patients be told about preventing exacerbations? • Avoid common triggers • Adhere to prescribed treatments • Use occlusive agents, emollients, and humectants • Provide and retain moisture in the skin • Enhance efficacy of topical corticosteroids and exert a steroid-sparing effect • Prevent disease exacerbation • Inhibit the Koebner response
What should patients be told about the risks of topical or systemic steroids? • Don’t use systemic steroids for psoriasis • Topical steroid side effects • Atrophy, telangiectasia, striae, acne • May exacerbate pre- / co-existing dermatoses • Can cause contact dermatitis • May lead to rebound • Limit superpotenttopicals (≤2x/d for ≤4wks, ≤50 g/wk) • Replace or combine with vitamin D analogues, retinoids, and calcineurin inhibitors • Increases efficacy with less steroid exposure
What behavior modifications can ameliorate the effects of psoriasis? • Stopping tobacco use • Reducing alcohol use • Maintaining ideal body weight
CLINICAL BOTTOM LINE: Patient Education… • Essential to optimizing treatment • Genetic + environmental factors contribute to psoriasis • Smoking, alcohol, obesity = more severe symptoms • Counsel patients on lifestyle modification • Individualized treatment regimen promotes adherence, improves treatment outcomes, and avoids toxicity