Psoriasis
Psoriasis . Diagnosis & Management Dr Rowan Brown February 2009. Pathogenesis. Hyperproliferation of keratinoctyes secondary to cytokine stimulus Epidermal thickening (acanthosis) Neutrophil/Lymphocyte infiltration Development of micro-abscesses in the corneum stratum

Psoriasis
E N D
Presentation Transcript
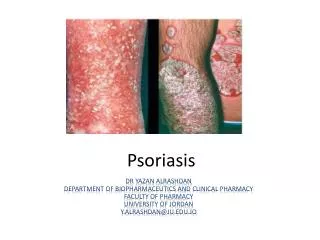
Psoriasis Diagnosis & Management Dr Rowan Brown February 2009
Pathogenesis • Hyperproliferation of keratinoctyes secondary to cytokine stimulus • Epidermal thickening (acanthosis) • Neutrophil/Lymphocyte infiltration • Development of micro-abscesses in the corneum stratum • Development of dilated capillaries in the dermis (resulting in bleeding points)
Histology hyperkeratosis microabscess
Aetiology • Immune mediated: antigen exposed within the corneum stratum • associated features • HLA CL6 (genetic) • Infection: Streptococcus → guttate psoriasis • Stress → exacerbations • Drugs → Alcohol, β-blockers +nsaids • Koebner Phenomenon (occurring in scar tissue)
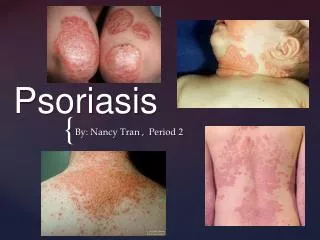
Clinical Features • 8 clinical subtypes • psoriasis vulgaris (most common) • guttate psoriasis (post infective) • flexoral psoriasis • erythrodermic psoriasis • palmoplantar psoriasis • psoriatic arthritis • nail psoriasis • acute pustular psoriasis
Acute Pustular Psoriasis • Widespread sterile pustules • These coalesce to form “lakes of pus” • Caused by withdrawl of steroids drugs, pregnancy • Septicaemia
Psoriasis Vulgaris (Plaque) • Common 0.5-3% of population • Single or multiple plaques • Age 15-40 (mean age 28yrs) • Extensor surfaces, back, sacrum, hairline, knees, elbows
Guttate Psoriasis • Multiple small lesions post infection • Often spontaneously resolve in 2-3/12 • Respond poorly to topical agents • Differential with pityriasis (scale confined to edge of lesions) pityriasis rosacea - scale confined to edge
Flexural Psoriasis • Typical eczema distribution • Often associated with psoriasis in the hair. • Differential with intertrigo
Erythrodermic Psoriasis • Results when 90% of body affected • Precipitated by withdrawl of steroids • Consequences: • infection • dehydration • high out-put cardiac failure
Palmoplantar Psoriasis • Vesicles on soles of hands & feet • Painful rather than itchy • Chronic condition
Psoriatic Arthritis • 5 main clinical subtypes: • symmetrical polyarthritis • asymmetrical oligoarthritis (large joint) • spondylitic (sero-negative) • distal-interphalangeal (nail) • severe mutilans
Nail Psoriasis • 50% of patients with skin involvement • 90% of psoriatic arthritis • pitting • onycholysis of distal nail bed • subungal hyperkeratosis
Treatment • Predominately benign + chronic condition • Topical/Systemic Treatments • Topical: - good for single isolated lesions • Tar - based preparations • Vitamin D-analogues • Steroids (rebound) • Dithranol (inhibits mitochondrial DNA)
Treatment • Systemic • UVB (nUVB = 311nm wavelength, is more effective) • PUVA = Psoralen + UV light • Useful for multiple lesions, erythrodermic psoriasis, pustular psoriasis • methotrexate (hepatic fibrosis + myelosuppression) • cyclosporin (hypertension, hypertrichosis, skin malignancy +lymphoma) • retinoids (good for pustular psoriasis)