Spirometry (Pulmonary Function Tests)
Spirometry (Pulmonary Function Tests). By: A. H. Mehrparvar, M.D. References. 1. M. R. Miller, et al. “ATS Standardisation of Spirometry”. Eur Respir J. 2005, 26: 319-338. 2. “Lung Function Testing: Selection of Reference Values and Interpretative Strategies”, ATS, 2003.


Spirometry (Pulmonary Function Tests)
E N D
Presentation Transcript
Spirometry (Pulmonary Function Tests) By: A. H. Mehrparvar, M.D.
References 1. M. R. Miller, et al. “ATS Standardisation of Spirometry”. Eur Respir J. 2005, 26: 319-338. 2. “Lung Function Testing: Selection of Reference Values and Interpretative Strategies”, ATS, 2003. 3. NIOSH Spirometry Training Guide, 2003. 4. Spirometry Handbook. National Asthma Council (Australia), 2004.
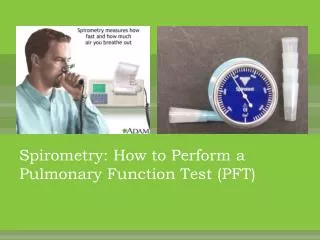
Definition A physiological test for measuring volumes inhaled or exhaled by an individual as a function of time
Indications • Not a screening test for general population • Diagnostic • Monitoring • Impairment evaluation • Public health
Indications (diagnostic) • Evaluation of symptoms and signs • Measuring the effect of dis. on pulmonary function • Screening individuals at risk for pulmonary dis. • Assess preoperative risk • Assess health status before physical activities (e.g. work)
Indications (monitoring) • Assess therapeutic intervention • Monitor people exposed to injurious agents
Spirometry standards • ATS (American Thoracic Society) • ERS (European Respiratory Society)
Spirometry maneuvers • FVC • VC and IC • PEF • MVV
FVC maneuver • Requirements of spirometer: • Accumulating volume for at least 15 s • Measuring volumes at least 8 lit (BTPS) • Accuracy of at least ± 3% or ±0.050 lit with flows between 0 and 14 lit/s • Showing both volume-time and flow-volume curves • Showing EV value
Test procedure • Maximal inspiration • A blast of exhalation • Complete exhalation to the end of test
Spirometric indices • FVC (forced vital capacity) • FEV1 (forced expiratory volume in 1 s) • FEV1/FVC • FEVt (forced expiratory volume in t s) • FEF25-75 (maximum midexpiratory flow) • PEF (peak expiratory flow)
Within maneuver evaluation • Start of test criteria - back extrapolation(EV < 5% of FVC or 150 ml) ● End of test criteria - the subject cannot or should not continue - exhalation at least 6s (in children under 10, 3s) - no change in volume (<0.025 lit) for at least 1s * In obstruction or older subjects more than 6s exhalation (till 15s)
Acceptability ● Start of test criteria ● End of test criteria ● cough especially during first second ● Valsalva maneuver (glottis closure) ● Leak from the mouth ● Obstruction of the mouthpiece ● Extra breath during the maneuver
Repeatability • At least three acceptable maneuvers Maximum difference between the largest and next largest FVC and FEV1 = 150ml (If FVC <1lit, this value is 100ml) ● At the most eight tests should be performed
Reversibility testing • Stop drugs (short-acting for 4 h, long-acting for 12h) before test • Stop smoking for 1 h. before test • Perform baseline test • Administer drug • Perform test after 10 – 15 min. (for salbutamol) or after 30 min. (for ipratropium)
Reversibility criteria 1. VC (forced or slow) and FEV1the primary indices for bronchodilator response. 2. A 12% increase, and a 200-ml increase in either FVC or FEV1 3. FEF25-75 should be used secondarily in evaluating bronchodilator response. 4. Ratios such as FEV1/VC should not be used to judge bronchodilator response.
VC maneuver • Two types (IVC and EVC) • Perform this test prior to FVC • Perform not more than 4 tests (at least 1 min. apart) • Surely use nose clip
Key Notes 1. be conservative in suggesting a specific diagnosisbased only on pulmonary function abnormalities. 2. Interpretborderline normal values with caution. 3. First step = to evaluate and comment on the quality of the tests.
Key Notes 4. The number of test indices (e.g., FVC, FEV1, etc.) used in interpretation shouldbe limited to avoid an excessive number offalse positive results. 5. The primary guides for spirometryinterpretation should be VC (slow or forced), FEV1, and FEV1/VC. 6. FEV1/VC should be the primary guide fordistinguishing obstructive from nonobstructive patterns.
Key Notes 7. If FEV1/VC is borderline, use Instantaneous and mid flows to confirm airway obstruction. 8. Don’t use FEF25-75 and the instantaneous flows to diagnose small airwaydisease. 9. The pattern of a low FEV1/VC and greater than average VC and FEV1 should be recognized as one that may occur inhealthy individuals.
Key Notes 10. The severity of airway obstruction shouldbe based on FEV1. 11. When FEV1 and FEV1/VC arenormal, don’t use FEF25-75 for grading the severity of obstruction. 12. A reducedVC and normal FEV1/VC suggest but not diagnose the presence of restriction. 13. The severity of restriction should be based on TLC. If VC is used, severity may be based on VC.
Lower Limits of Normal 1. Normal ranges should be based on calculated fifth percentiles. 2. Lower limits of normal are variable. 3. The use of 80% of predicted for adult pulmonary function parameters is not recommended. This criterion works only for average persons and for a limited number of parameters.
LLN • FEV1 and FVC = 80% • FEV1/FVC = 70-75% • FEF25-75 = 50-60%
Interpretation A. Normal: both the VC and the FEV1/VC ratio are normal. B. Obstructive: FEV1/VC ratio is below the normal range. The severity of the abnormality is graded: - % Pred FEV1 > 100 = May be a physiological variant - % Pred FEV1 < 100 and > 70 = Mild - % Pred FEV1 < 70 and > 60 = Moderate - % Pred FEV1 < 60 and > 50 = Moderately severe - % Pred FEV1 < 50 and > 34 = Severe - % Pred FEV1 < 34 = Very severe
Interpretation C. Restrictive: This is most reliably interpreted on the basis ef TLC. If this is not available,one may interpret a reduction in the VC without a reduction of the FEV1/VC ratio as a restriction The severity of the abnormality might be graded as follows: -% Pred VC < LLN and > 70 = mild - % Pred VC < 70 and > 60 = Moderate • % Pred VC < 60 and > 50 = Moderately severe • % Pred VC < 50 and > 34 = Severe - % Pred VC < 34 = Very severe
IC ERV RV TLC TLC VC Vt VC FRC RV RV Normal
Vital capacity is reduced in both obstructive and restrictive diseases VC VC VC RV RV RV Obstructive Normal Restrictive
An Algorithm for Spirometry Is maneuver acceptable? n o y e s Is the FEV1/FVC lower than predicted? Interpretation may be limited by falsely low FVC n o y e s This is the definition of obstruction Mild FEV1 >70% Moderate FEV1 60-70% Mod severe FEV1 50-60% Severe FEV1 <50% Very severe FEV1 <40% Is FVC reduced? n o y e s Restriction may be present; Need TLC to definitively diagnose restriction Normal pulmonary mechanics Restriction Lung volumes: Spirometry: Severity determined by Severity is determined the reduction in TLC by the reduction in VC Mild 65-80% Mild 70-80% Moderate 50-65% Moderate 60-70% Severe <50% Severe <60%
Case 1 • A 38 year-old male • Height: 171, weight: 82 • FVC = 4.53 (100%) • FEV1 = 3.35 (89%) • FEV1/FVC = 74% • FEF25-75 = 2.85 (65%)
Case 2 • A 53 year-old male • Height: 180, weight: 73 • FVC = 4.51 (97%) • FEV1 = 3.18 (86%) • FEV1/FVC = 70.50% • FEF25-75 = 2.26 (58%)
Case 3 • A 41 year-old male • Height: 171, weight: 65 • FVC = 4.77 (115%) • FEV1 = 3.50 (101%) • FEV1/FVC = 73.40% • FEF25-75 = 2.74 (66%)
Case 4 • A 52 year-old male • Height: 181, weight: 95 • FVC = 3.81 (81%) • FEV1 = 2.38 (63%) • FEV1/FVC = 62.5% • FEF25-75 = 1.72 (41%)
Case 5 • A 39 year-old male • Height: 184, weight: 83 • FVC = 5.82 (111%) • FEV1 = 4.98 (116%) • FEV1/FVC = 85.6% • FEF25-75 = 5.25 (114%)
Case 6 • A 44 year-old male • Height: 185, weight: 92 • FVC = 3.93 (76%) • FEV1 = 2.75 (66%) • FEV1/FVC = 70% • FEF25-75 = 1.91 (43%)
Case 7 • A 54 year-old male • Height: 178, weight: 80 • FVC = 4.56 (121%) • FEV1 = 3.10 (102%) • FEV1/FVC = 68% • FEF25-75 = 1.83 (51%)