Download
1 / 14
140 likes | 275 Views
Thorny Issues in HIV Vaccine Trials. Saul Walker Policy Advisor IAVI. Thorny Issues?. Vaccine positivity (including insurance) Clades Partial efficacy and end-points Cohort selection Phase 2b or not Phase 2b Placebo selection

E N D
Thorny Issues in HIV Vaccine Trials Saul Walker Policy Advisor IAVI
Thorny Issues? • Vaccine positivity (including insurance) • Clades • Partial efficacy and end-points • Cohort selection • Phase 2b or not Phase 2b • Placebo selection • Standards of Care for trial participants in developing countries
Vaccine positivity • Vaccines often intended to induce antibodies • Standard HIV tests may show +ve for vaccine induced response • Possible to determine true and vaccine positivity through selective tests, such as PCR • Volunteers provided with information and directions for future testing • Insurance • ABI recognised issue of vaccine positivity • Assumptions that volunteers are ‘high risk’
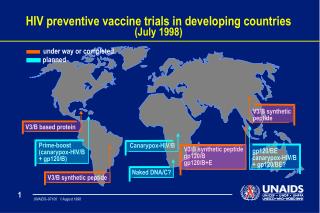
Clades • Genetic variability in HIV produced numerous clades
Clades • Genetic variability in HIV produced numerous clades • Variability challenging for vaccine design but don’t know how important clade issue is • Animal data showing cross reactivity for a number of candidates • Only clinical data will be conclusive • Potential for multi-clade vaccines • VRC has an ABC product • Some parts of virus relatively well conserved • Broad protection a key objective
Efficacy • Types of Immunity • Sterilising Immunity (Vs): protection from infection • Disease mitigation (Vp): infection but delays or prevention of disease progression • Reduced Infectiveness (Vi): lower VL leading to reduced transmission • End points • For Vp focus has been on viral set point and/or time to treatment • Vi more difficult to design ethical trial • Limited Efficacy • Some of the people all of the time or all of the people some of the time • Efficacy and Effectiveness: potential for behavioral reversals
Cohort Selection • Adolescents • A key group that could benefit from a vaccine • Consent issues and parental sensitivities • Discordant couples • Treatment for positive partner? • Possible European cohorts • Vulnerable groups • IDUs, sex workers, MSMs …. Service men/women etc • Adding to existing stigma
Phase 2b Trials • Need to accelerate development and time to field while managing investment risks • Novel trial designs and strategies • Phase 2b - ‘Proof of concept’ • Shorter trial designed to show efficacy > 0 • Expand into Phase 3 trial for license • Reduces initial trial costs but can increase total time • Reduces manufacturing investment risks • Designs that expand into Phase 3
Placebo Selection • Compare gold standard with gold standard + vaccine • Under trial conditions, gold standard can dramatically reduce incidence • Availability of limited efficacy vaccines could make trials impractical • Phase 2b to Phase III transition? • Availability of new prevention options, such as microbicides
Standards of Care in Developing Countries • Trial participants package of care including primary care and HIV prevention • Treatment beyond trial not an ethical obligation for prevention trials • ‘morally praiseworthy’ • Emerging consensus of ‘how’ not ‘if’ • Practical issues: who, when, how long, ensuring provision, cost • Agreement on shared responsibilities • Sustainability • Trial/community disparities
Standards of Care in Developing Countries • Consultation essential • Policy development evolved in discussion with WHO-UNAIDS, other sponsors, researchers and NGOs • IAVI undertaken consultations in Uganda and India consultations
IAVI SOC Policy - Commitments • Ongoing consultation on detail and implementation • Support primary healthcare and HIV prevention services to an agreed standard for trial participants for the duration of the trial* • Support access to treatment, care and support, including ART when recommended by treatment guidelines, for participants who become HIV infected during a trial* • Initial commitment of 5ys ART after start of treatment recommended • Funding for therapy through an Escrow Account or appropriate national scheme. • Treatment guidelines will be agreed with country stakeholders before trial initiation with WHO guidelines providing a baseline • IAVI will ensure referral to local support services for volunteers who are HIV-infected and who are screened out before enrolment *unless sufficiently covered under and existing national programme
IAVI SOC Commitments • IAVI will work actively with country and international stakeholders to support opportunities for trial related investments to provide benefit to communities in which trials take place • Capacity building • Link trial activities with local HIV/AIDS programmes and health services • IAVI will work with country and international stakeholders to support; • Sustained provision of treatment, care and support for trial participants who have become HIV infected during a trial • Opportunities to build on trial related investments to provide sustained community health benefits