Complex Coronary Cases
Complex Coronary Cases. Supported by: Abbott Vascular Boston Scientific Corporation Medtronic, Inc. Astrazeneca. Disclosures. Samin K. Sharma, MBBS, FACC Speaker’s Bureau – Boston Scientific Corporation, Abbott, The Medicines Company, Daiichi Sankyo, Inc. and Lilly USA, LLC

Complex Coronary Cases
E N D
Presentation Transcript
Complex Coronary Cases Supported by: Abbott Vascular Boston Scientific Corporation Medtronic, Inc. Astrazeneca
Disclosures Samin K. Sharma, MBBS, FACC Speaker’s Bureau – Boston Scientific Corporation, Abbott, The Medicines Company, Daiichi Sankyo, Inc. and Lilly USA, LLC Annapoorna S. Kini, MBBS, FACC Nothing to disclose Sameer Mehta, MBBS, FACC Consulting Fees – The Medicines Company American College of Cardiology Foundation staff involved with this case have nothing to disclose
April 16th 2013 Case #10: SA, 53 yr M Presentation: Presented on 2/26/2013 with vague chest pain with nonspecific pre-cordial T wave changes associated with variable dyspnea. Stress test suggested but declined and underwent cath revealing one vessel CTO (mLAD) with LVEF 56%. No PCI done as was inappropriate; not on any anti-ischemic meds and no documented ischemia. Pt was placed on Metoprolol XL 25mg and Amlodipine 5mg daily. A F/U stress MPI revealed moderate size large antero-lateral and apical ischemia. Still has residual class I-II angina. Prior History: Hyperlipidemia, NIDDM, Ex-smoker, +F/H, H/o RA Medications: All once daily dosage Aspirin 81mg, Metoprolol XL 25mg, Amlodipine 5mg, Metformin XL 1000mg, Rosuvastatin 20mg, Methotrexate, Sulfasalazine
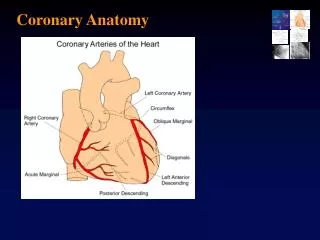
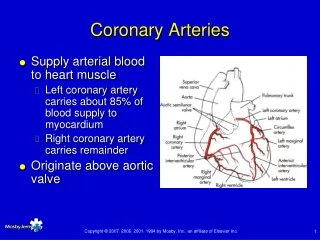
Case# 10: cont… SYNTAX score 19.5 Cardiac Cath 2/26/2013: Right Dominance 1 Vessel CAD with LVEF 56% (minimal apical hypokinesis) Left Main: Short LAD: 100% lesion in mid and distal fills via RCA and bridge collaterals, 90% D1 LCx: Non-obstructive RCA: No obstruction Plan Today: - PCI of CTO mid LAD via antegrade or retrograde approach
Issues Involving The Case • Predictors of CTO lesion success • Correlation of IVUS, OCT and FFR
Predictors of Procedural Success Multivariate analysis from TOAST-GISE Olivari et al., J Am Cardiol Coll 2003;41:1672
Incidence of Procedural Complications in Successful vs. Unsuccessful CTO PCI Complications Successful Unsuccessful p value Patel et al., JACC Cardiovasc Interv 2013;6:128
Temporal Trends in Cumulative Angiographic Success Rates and Major Procedural Complication Rates 80% 0.5% Patel et al., JACC Cardiovasc Interv 2013;6:128
Predictors of Reocclusion After Successful Drug-Eluting Stent-Supported Percutaneous Coronary Intervention of Chronic Total Occlusion: Florence CTO PCI Registry Valenti et al., J Am Coll Cardiol 2013;61:545
CTO PCI Registry: Clinical and Angiographic Outcomes First-Generation DES vs. Second-Generation EES (N= 802) Valenti et al., J Am Coll Cardiol 2013;61:545 * p = 0.001
CTO PCI Outcomes: Predictors of Clinical and Angiographic Outcome Valenti et al., J Am Coll Cardiol 2013;61:545
CTO PCI Outcomes: 3 Years MACE Free Survival Based on the Technique P = 0.014 nonSTAR STAR Valenti et al., J Am Coll Cardiol 2013;61:545
Use of Novel Crossing and Re-Entry System in Coronary CTOs Failing Standard Crossing Techniques Stingray Re-Entry Balloon Catheter and Guidewire CrossBoss Crossing Catheter Whitlow et al., JACC Cardio Interv 2012;5:393
CTO Dissection/Re-entry Strategies CTO dissection/re-entry strategies Retrograde Antegrade Re-entry Dissection Dissection Re-entry • STAR • Contrast-guided STAR • mini-STAR • LAST • Stingray Knucle wire • Knucle wire • CrossBoss • CART • Reverse Cart
Issues Involving The Case • Predictors of CTO lesion success • Correlation of IVUS, OCT and FFR
Schematic representation of various functional hemodynamic measurements Microvasculature Microvasculature OCT Microvasculature Criteria for significant stenosis: IVUS = <4mm2 FFR = <0.8 OCT = ?
FIRST Study: Fractional Flow Reserve and Intravascular Ultrasound Relationship Study 10 US/European centers enrolled 350 pts (367 lesions) with intermediate angiographic lesions (40-80%) and underwent IVUS, VH and FFR Waksman et al., JACC 2013;61:917
FIRST Study Scatterplots of IVUS MLA and FFR Correlation: Infarct of Vessel Size (RVD) All Vessels RVD <3.0mm 2.68 mm2 3.07 mm2 RVD 3-3.5mm RVD >3.5mm 3.74 mm2 3.16 mm2 Waksman et al., JACC 2013;61:917
FIRST Study: Diagnostic Accuracy of IVUS MLA in Prediction of Functionally Significant Stenosis and by RVD sensitivity specifity ppv npv % Waksman et al., JACC 2013;61:917
FIRST Study: Scatterplots of IVUS and FFR All lesions that underwent PCI with FFR of 0.8, MLA of 3.07 mm2 All lesions that did not undergo PCI with FFR of 0.8 and MLA of 3.07 mm2 Waksman et al., JACC 2013;61:917
OCT vs IVUS Assessment of Native Coronary Artery Disease p=0.294 IVUS (56) FD-OCT (56) p=<0.001 p=0.226 p=<0.001 Bezzera et al., JACC Cardiovasc Interv 2013;6:228
OCT vs. IVUS Assessment of Stented Vessels Post PCI and at Follow Up Bezzera et al., JACC Cardiovasc Interv 2013;6:228
VIRTU-1 Study: Example of vFFR in a Left Anterior Descending Artery Morris et al., JACC Cardiovasc Interv 2013;6:149
DeFACTO Study: Per-Patient Diagnostic Performance for Intermediate Stenoses by CT (30-70%)
Take Home Message:Predictors of CTO success and Correlation of various non-invasive studies • In the current era of CTO recanalization, angiographic predictors of failure are few, important being heavy Ca++. Subintimal tracking is associated with high reocclusion rates and hence should be avoided. Unsuccessful recanalization is still associated with higher MACE rates • Recent data suggest IVUS lumen CSA of 3.1mm2 to correlate with FFR of <0.8 and is dependent on RVD. OCT provides on an average 1mm smaller lumen area compared to IVUS & hence OCT criteria for hemodynamic significant lesion may be different then IVUS
Question # 1 • Following are the predictors of successful recanalization of the CTO lesions except : • Tapered end • Heavy calcification • No bridge collaterals • Short occlusion (8-15mm)
Question # 2 • A recent multicenter registry showed current success of CTO to be : • <50% • 50-70% • 71-85% • >85%
Question # 3 • Following observation about FFR and IVUS correlation was noted in the FIRST study : • A. There is a fixed relationship with RVD and FFR of <0.8 • B. There is a good correlation of IVUS MLD and FFR • FFR cutoff of 0.8 will lead to less PCI vs. IVUS MLD cutoff • VH parameters on IVUS correlate well with FFR of <0.8
Question # 1 • Following are the predictors of successful recanalization of the CTO lesions except : • Tapered end • Heavy calcification • No bridge collaterals • Short occlusion (8-15mm) The correct answer is B. Heavily calcified lesions are associated with lower success of CTO recanalization Olivari et al., J Am Cardiol Coll 2003;41:1672
Question # 2 • A recent multicenter registry showed current success of CTO to be : • <50% • 50-70% • 71-85% • >85% The correct answer is C. Recent multicenter CTO registry demonstrated increasing success of CTO recanalization over the years with latest being over 80% Patel et al., JACC Cardiovasc Interv 2013;6:128
Question # 3 • Following observation about FFR and IVUS correlation was noted in the FIRST study : • A. There is a fixed relationship with RVD and FFR of <0.8 • B. There is a good correlation of IVUS MLD and FFR • FFR cutoff of 0.8 will lead to less PCI vs. IVUS MLD cutoff • VH parameters on IVUS correlate well with FFR of <0.8 The correct answer is C. FIRST study showed that FFR and IVUS MLD has poor correlation and is dependent on RVD. FFR cutoff of 0.8 will lead to less PCI compared to any IVUS MLD cutoff even of 3.1mm2 Waksman et al., JACC 2013;61:917