Complex Coronary Cases
Complex Coronary Cases. Supported by: Abbott Vascular Boston Scientific Corporation Medtronic, Inc. AstraZeneca St Jude’s Medical Abiomed Vascular solution Bracco Diagnostic. Disclosures. Samin K. Sharma, MBBS, FACC

Complex Coronary Cases
E N D
Presentation Transcript
Complex Coronary Cases Supported by: Abbott Vascular Boston Scientific Corporation Medtronic, Inc. AstraZeneca St Jude’s Medical Abiomed Vascular solution Bracco Diagnostic
Disclosures Samin K. Sharma, MBBS, FACC Speaker’s Bureau – Boston Scientific Corporation, Abbott Vascular Inc, AngioScore, The Medicines Company, Daiichi Sankyo, Inc. and Lilly USA, LLC Annapoorna S. Kini, MBBS, FACC Nothing to disclose Sameer Mehta, MBBS, FACC Consulting Fees – The Medicines Company American College of Cardiology Foundation staff involved with this case have nothing to disclose
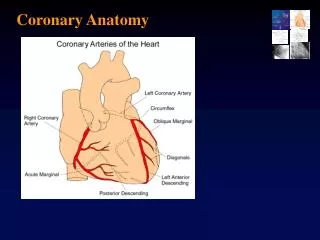
Nov 19th 2013 Case #17: WR, 73 yr M Presentation: Patient presented with new onset exertional angina class II and positive high risk MPI for large infero-lateral and inferior ischemia. Cardiac cath on 10/21/13 revealed 3 V CAD (90% D1, 100% moderate size OM1 and 100% prox RCA with extensive collaterals from LAD/LCx) and LVEF 60%. Syntax score 21. Patient underwent EES DES x2 to D1. Pt still continued exertional angina despite MMT Prior History: Hypertension, Hyperlipidemia, +F/H Medications: All once daily dosage Metoprolol XL 50mg, ISMN 30mg, Losartan/HCTZ 50/25mg, ASA 81mg, Clopidogrel 75mg, Simvastatin 80mg
Case# 17: cont… Cardiac Cath 10/21/2013: Right Dominance 3 V CAD with LVEF 60% Left Main: No obstruction LAD: 30% pLAD and 90% calcific D1 LCx: 100% OM1 moderate size RCA: 100% pRCA, distal vessel large and fills via LAD/LCx collaterals Pt underwent PCI using 2 EES DES (2.5/23 and 2.5/12mm) of D1 with excellent results. Pt was discharged same day. Pt continued to have exertional angina despite MMT Plan Today: - PCI of CTO RCA using antegrade or retrograde approach
Issues Involving The Case • Recent Trials of Coronary Bifurcation • Lesion PCI • Update in Duration & DAPT Interruption • post- DES
Issues Involving The Case • Recent Trials of Coronary Bifurcation • Lesion PCI • Update in Duration & DAPT Interruption • post- DES
Coronary Artery Bifurcation Lesion Interventional Techniques Interventional Bifurcation Techniques One Stent Technique (OST) Crush Stent Technique (CrST) Kissing Stent Technique (SKS) ‘T’ Stent Technique (TST) OST with SBR Dilatation (SBT) Culotte Stent Technique (CUT)
Bifurcation Lesion Intervention: 1 vs. 2 Stents Technical Issues • One stent (ok & simple but may have difficulty • in rewiring or inserting second stent as bailout) • or 2 stents (guaranteed coverage of both lesions but higher MACE, TVR or ST in many studies) • If 2 stents; ?technique
A Randomized Clinical Study Comparing Double Kissing Crush With Provisional Stenting for Treatment of Coronary Bifurcation Lesions: DK Crush II Study Conventional (n= 185) p<0.001 % DK Crush (n=185) 22.2 p=0.017 p=0.07 17.3 14.6 p=0.036 10.3 9.7 p=0.37 6.5 4.9 3.8 2.2 0.5 ST Main Vessel Side Vessel MACE TVR Angiographic Restenosis Chen S et al, JACC 2011;57:914
Nordic-Baltic Bifurcation Study IV: Patient Flow Chart Nordic Baltic Bifurcation study IV n=450 Provisional SB stening n=221* Two stent n=229* 1 lost to FU 1 excluded due to protocolviolation 1 withdrawal Provisional Completed 6M FU n=220 Two stent Completed 6M FU n=227 Kumsars et al., TCT 2013
Nordic-Baltic Bifurcation Study IV: Procedural Data *Residual stenosis <30% of MV + TIMI flow III in SB Kumsars et al., TCT 2013
Nordic-Baltic Bifurcation Study IV: Procedural Data *Residual stenosis <30% of MV + TIMI flow III in SB **Assessment possible in 327 patients Kumsars et al., TCT 2013
Nordic-Baltic Bifurcation Study IV: Event Free Survival Curve at 6 Months 1.8% 4.6% p=0.09 Kumsars et al., TCT 2013
Nordic-Baltic Bifurcation Study IV: Individual Endpoints at 6 Months Provisional (n=220) p=0.11 Two-stent (n=227) p=0.39 % p=0.50 p=0.54 p=0.32 Kumsars et al., TCT 2013
TRYTON Bifurcation Trial: Study Design Baseline Angiography – Eligible for Randomization TRYTON side branch + DES (main vessel) DES (main vessel) + Provisional side branch N = 704 TVF PrimaryEndpoint Clinical F/U at 9 months Clinical F/U at 9 months %DS side branch (N=374) Secondary Endpoint Angiographic F/U at 9 months Angiographic F/U at 9 months IVUS Cohort n~96 IVUS F/U at 9 months IVUS F/U at 9 months Leon et al., TCT 2013
TRYTON Bifurcation Trial: Patient Flow Randomized N=704 TRYTON + DES N=355 Provisional + DES N=349 9 Month Follow-up N=681 TRYTON = 345 Provisional = 336 Provisional 6=LosttoF/U 5=Patientwithdrawal 4= Death TRYTON 4=LosttoF/U 2=Patientwithdrawal 4= Death Angiographic N=326 TRYTON = 158 Provisional = 168 IVUS N=94 TRYTON = 59 Provisional = 35 • Clinical FU at 9 months = 97% • Angiographic FU at 9 months = 87% Leon et al., TCT 2013
TRYTON Bifurcation Trial: TVF at 9 Months Primary Endpoint TRYTON (N=355) 17.4% Difference 4.6% Upper 1- Sided 95% CI 10.3% Non-inferiority p value = 0.4167 Provisional (N=349) 12.8% Zone of non-inferiority pre-specified margin = 5.5% Non-inferior 0 1.0 2.0 4.0 5.0 6.0 7.0 8.0 9.0 10.0% 11.0 3.0 Primary Non-Inferiority Endpoint Not Met Leon et al., TCT 2013
TRYTON Bifurcation Trial: TVF Primary Endpoint ST 0.3% 0.6% Provisional S (N=349) TRYTON S (N=355 p =0.108 p =0.109 % p =0.564 Non-Hierarchical Leon et al., TCT 2013
TRYTON Bifurcation Trial: Additional Side Branch Stents Indications Provisional TRYTON % Leon et al., TCT 2013
TRYTON Bifurcation Study: SB %DS (In-segment) Secondary Endpoint p=0.002 % Secondary Superiority Endpoint Met Leon et al., TCT 2013
COBIS II Registry: Independent Predictors of Side Branch Occlusion (Occurs in 8.4% cases) Hahn et al., JACC 2013;62:1654
COBIS II Registry: Clinical Outcomes at 1-Yr F/U Of the 187 SBr occlusion 31% of SBr occlusion remained post PCI p=0.03 SB Occlusion (n=187) No SB Occlusion (n=2040) p=0.36 % p=0.002 p=0.002 p=0.46 Hahn et al., JACC 2013;62:1654
Issues Involving The Case • Recent Trials of Coronary Bifurcation • Lesion PCI • Update in Duration & DAPT Interruption • post- DES
Optimal Duration of ADP Receptor Blockers Post DES Still Remain Unclear (Aspirin 81-325 mg daily for life) AHA/ACC Updated Guidelines 2006 Cypher Stent Launch 5/2003 AHA/ACC/SCAI Updated Guidelines 2005 CURE, PCI-CURE – 2001 CREDO – 2002 (TAXUS stent 6 months post PCI) (Cypher stent 3 months post PCI) 9-12 months (FDA recommendations) Clopido/Prasugrel/Ticag should be continued for 1 yr or even longer if no contraindications DES Era BMS Era AHA/ACC PCI Guidelines 2001 TAXUSStent Launch 3/2004 ESC 2005/ACC 2006 PCI Updated Guidelines (12 months post PCI) (1-12 months post BMS) If not sure about DAPT compliance or has to be interrupted in 12M then BMS (Basket late) is safer & should be preferred
Randomized Trials of DAPT Duration MACE Bleeding % REAL-LATE RESET PRODIGY
OPTIMIZE Trial: Study Design Broad patient population undergoing PCI with Endeavor ZES RVD 2.5 mm – 4.0 mm 12 Months DAPT N = 1560 3 Months DAPT N = 1560 N = 3120 patients 1:1 Randomization 33 Sites in Brazil Clinical endpoints 30-d. 3-mo. 6-mo. 12-mo. 18-mo. 24-mo. 36-mo. Primary Endpoint: NACCE (Death / MI / Stroke / Major Bleeding) at 12 months Secondary Endpoints: ARC defined ST, TVR, TLR, MACE, DAPT compliance, and major bleeding (REPLACE-2 & GUSTO definitions) NACCE = Net Adverse Clinical and Cerebral Events MACE is composed of Death, MI, Emergent CABG, TLR Feres et al., Am Heart J 2012;164:810
OPTIMIZE Trial: DAPT Usage 3 Months DAPT (N=1563) 12 Months DAPT (N=1556) Patients on DAPT (%) Time After Initial Procedure Feres et al., TCT 2013
OPTIMIZE Trial: NACCE at 1 Year (All-Cause Death, MI, Stroke, Major Bleeding) 15 3MDAPT 12M DAPT 10 Non-inferiority P-value = 0.002 Cumulative Incidence of NACCE (%) 6.0 Log-Rank P = 0.84 HR 1.03 (0.77 – 1.38) 5.8 5 0 0 3 6 9 12 Time After Initial Procedure (Months) Feres et al., TCT 2013
OPTIMIZE Trial: Other Clinical Events at 1 Year 3 Months DAPT (N=1563) 12 Months DAPT (N=1556) p=0.36 Events (%) p=0.49 p=0.70 p=0.47 p=0.82 p=0.41 p=0.99 Feres et al., TCT 2013
ARCTIC-Interruption Study: Flow Chart Rd#1: 2440 patients in ARCTIC 1181 were excluded Rd#2: 1259 randomized by IVRS one year after stenting 635 DAPT FOR ITT ANALYSIS 624 SAPT FOR ITT ANALYSIS 6-18 months of Follow-up death, MI, stroke, stent thrombosis, or urgent revascularization Montalescot, TCT 2013
ARCTIC-Interruption Study: All Ischemic Endpoints DAPT (N= 635) p=0.57 SAPT (N= 624) p=0.52 % p=0.58 p=0.58 p=0.74 p=0.94 p=0.56 Primary ST or urg. Death Any death MI ST Stroke Urgent Endpoint* revasc or MI or TIA revasc *Any death, MI, ST, Stroke or TIA, Urgent revasc Montalescot, TCT 2013
ARCTIC-Interruption Study: Key Safety Outcome DAPT (N= 635) p=0.03 SAPT (N= 624) p=0.07 % p=0.07 p=0.29 Montalescot, TCT 2013
DAPT DURATION POST DES • Therefore DAPT duration of 6M (?3M) is now becoming the new 12M with newer generation DES What about DAPT discontinuation POST DES?
Xience V USA Registry: Late ST Rates (30 D – 1 Year) After DAPT Interruption Overall Standard (Low) Risk Subsequent Late ST (ARC Def/Prob) (%) 0.49 0.37 0.26 0.16 0 0 0 0 13/3500 2/1272 2/435 0/157 1/378 0/147 0/292 0/120 No Interruption Interruption After 30 Days Interruption After 180 Days Interruption After 90 Days Krucoff, Hermiller, Sharma et al. JACC Intervent 2011;4:1298.
Modes of DAPT Cessation • Discontinuation • patients had discontinued DAPT as per recommendation of their physician who felt the patient no longer needed therapy • Interruption • patients had interrupted DAPT use on a voluntary basis and as guided by a physician due to (e.g. surgery) • DAPT was then reinstituted within 14 days • Disruption • patients had disrupted DAPT use due to bleeding or non-compliance.
PARIS Study: 2-Year K-M Plot of Any DAPT Cessation 60 Two Years (57.3%) 50 40 Cumulative Incidence, % 30 One Year (23.3%) 20 10 30 Days (2.9%) 0 6 12 18 24 Time since PCI, Months
PARIS Study: 2-Year Kaplan-Meier Plots of Any Discontinuation, Interruption and Disruption 60 Discontinuation Disruption Interruption 50 40.8% 40 Cumulative Incidence, % 30 14.4% 20 10.5% 10 0 6 12 18 24 Time since PCI, Months
PARIS Study: DAPT Cessation and MACE P Events (n) HR (95% CI) On-DAPT 1.00 (Ref) 413 Discontinuation 0.63 (0.46, 0.86) 0.004 52 Interruption 1.41 (0.94, 2.12) 0.101 26 Disruption 1.50 (1.14, 1.97) 0.004 67 7.04 (3.31, 14.95) <0.001 7 0-7 Days 8-30 days 2.17 (0.97, 4.88) 0.06 6 31+ days 1.30 (0.97, 1.76) 0.083 54 0.25 0.5 1 2 4 8 16 Hazard Ratio Mehran et al., TCT 2013
PARIS Study: DAPT Cessation and Def/Prob Stent Thrombosis HR (95% CI) P 1.00 (Ref) On-DAPT 0.39 (0.11, 1.35) Discontinuation 0.64 (0.09, 4.82) Interruption 2.58 (1.22, 5.46) Disruption 15.94 (5.57, 45.58) <0.001 0-7 Days 2.68 (0.36, 19.68) 0.334 8-30 days 1.35 (0.50, 3.64) 0.551 31+ days 0.25 0.5 1 2 4 8 16 32 64 Hazard Ratio Mehran et al., TCT 2013
Dual Antiplatelet Therapy (DAPT) Study 12 months 18 months DES n= 15245 BMS n=5400 All patients on aspirin + open-label thienopyridine therapy for 12 months 1:1 Randomization at 12 months 50% of patients continue o dual antiplatelet therapy (clopidogre or prasugrel) 50% of patients receive aspirin + placebo Total 33-month patient evaluation including additional 3-month follow-up Mehran et al., TCT 2013
Take Home MessageTrials of Bifurcation Lesions and DAPT duration/Interruption • Trials of large bifurcation lesion interventions have suggested favorable outcomes with 2S vs. 1S strategy without higher ST. Dedicated TRYTON bifurcation (BMS) stent was not superior to provisional stent approach • Trials of DAPT duration post DES support a shorter (3-6M) vs. 1+ year with lower bleeding and similar MACE. Hence 6M (?3M) DAPT duration should be routine post DES. Also physician directed DAPT interruption post DES is not associated with adverse outcomes
Question # 1 • Which of the following trial compared 6M vs. 24M of DAPT duration: • PARIS Study • PRODIGY Trial • REAL LATE Trial • OPTIMIZE Trial • RESET Trial
Question # 2 • TRYTON bifurcation trial showed the following superior results • over provisional stent strategy : • Lower TVR • Lower MI • Lower SBr %DS • Lower stent thrombosis • Higher CVA
Question # 3 • Sidebranch occlusion post PCI is associated with the following except : • A. Higher mortality • B. Higher MI • C. Higher Stent thrombosis • D. Lower TVR • E. Higher MACE