Download
1 / 29
330 likes | 572 Views
Preliminary Analysis Of Phase I, First-In-Human, Cathepsin Activated Tumor Imaging Probe Brian Brigman November 1, 2013. 1. Disclosures. Patent for imaging device held by MIT and Duke Lumicell Diagnostics Scientific Advisory Board (DK) Own Stock (DK, JF) Employee (JF)

E N D
Preliminary Analysis Of Phase I, First-In-Human, Cathepsin Activated Tumor Imaging Probe Brian Brigman November 1, 2013 1
Disclosures • Patent for imaging device held by MIT and Duke • Lumicell Diagnostics • Scientific Advisory Board (DK) • Own Stock (DK, JF) • Employee (JF) • Preclinical research supported by: • NSF (DK, WE) • NCI SBIR (Subcontract - BB) • CTSA (BB) • Phase I study supported by • ASCO Advanced Clinical Research Award (DK)
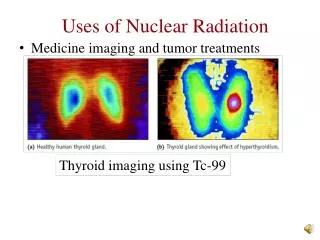
What is the problem? • Local recurrence of soft tissue sarcoma after wide resection • Presumably due to residual tumor left in tumor bed • We use margin assessment as a surrogate for our real question – is there tumor left in the tumor bed?
What is the problem? • Multiple studies of surgery alone for high grade STS show recurrence rates of 30-40% • Prospective trial of surgery alone for STS • Pisters et al. JCO 1996 • + Margin: Recurrence 5/14 (36%) • - Margin: Recurrence in 20/72 (28%)
Isn’t that what Radiation is for? • Radiation does decrease local recurrence significantly • Morbidity of radiation therapy • O’Sullivan et al. Lancet 2002 • Davis et al. RadiotherOnc2005 • Fibrosis/Edema • Osteonecrosis/Fracture • Radiation associated malignancy • Wound healing complications
Who needs radiation? • “Wide” Resection alone • ~66% local control in high grade sarcoma • Radiation Therapy with Surgery • ~10% recurrence with surgery and radiation Only 25% of patients benefit from Radiation
Optical Imaging of Microscopic Residual Cancer • A system for intra-operative margin assessment that can detect microscopic residual disease within the tumor bed • If successful: • Intensify therapy for patients with residual cancer • Minimize RT for patients with no residual cancer • Reduce rates of repeat resection
Multiple Cathepsin Proteases are Overexpressed in Soft Tissue Sarcomas Sarcomas Muscle (Mito JK, et al. Cancer 2012) (Cuneo KC, et al. IJROBP 2013) 8
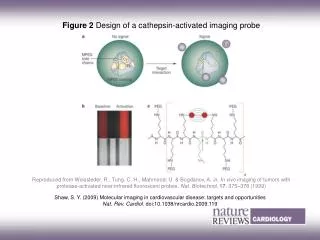
LUM015 NIR Fluorescent Probe QUENCHER Cathepsin Cleavage Site PEG MW~22,000 g/mol CY5 FLUOROPHORE 10
Intraoperative Imaging System (Mito JK, et al. Cancer 2012) 11
Tumor and Tumor Bed Imaging in Genetically Engineered Mouse model of Soft Tissue Sarcoma (Mito JK, et al. Cancer 2012)
Genetically Engineered Mouse Model of Soft tissue Sarcoma treated with surgery alone with or without Fluorescent imaging Intra-operative Fluor Imaging Standard Margin Assessment 13
De novo Canine tumor imaging trial data (mean f/u >1 year) (EwardWE et al. CORR) 2012
A Phase I Study of the Safety and Activation of a Cathepsin-Activatable Fluorescent Probe LUM015 Primary Objective To determine a safe and recommended phase II intravenous dose of LUM015 that labels tumors in human patients with sarcoma. Secondary Objectives To obtain imaging data of the tumor and any adjacent normal appearing tissue in pathology suite – No imaging of patient tumor beds To obtain PK/PD data regarding LUM015 when administered IV in patients To analyze cathepsin protease expression in tumors. Modified 3+3 design with up to 3 dosing levels Starting probe dose (0.5 mg/kg) and time to tumor visualization (>24 h) based on allometric scaling from mouse data and mathematical simulations of Lum015 in humans 15
Mathematical Simulations of LUM015 Revision 15: 4/2/2012 16
17 Trial stops w/o safe dose for future phase II studies Trial stops w/o safe dose for future phase II studies 1.0 mg/kg is established as a safe dose for future phase II studies Decrease Dose: 3 @ 0.25 mg/kg Dose Expansion: 3@ 0.25 mg/kg 0.25 mg/kg is established as a safe dose for future phase II studies START HERE 3 @ 0.5 mg/kg ≥1 subjects with adverse pharmacologic activity No subjects with adverse pharmacological activity Decrease Dose: 3@ 1.0 mg/kg Increase Dose: 3 @ 1.0 mg/kg Decrease Dose: 3@ 1.0 mg/kg Increase Dose: 3 @ 1.5 mg/kg 1.5 mg/kg is established as a safe dose for future phase II studies Dose Expansion: 3 @ 1.5 mg/kg 1.0 mg/kg is established as a safe dose for future phase II studies
Dose Escalation 3/3 3/3 No Adverse Pharmacological Events 18
38 year old female with biopsy proven UPS s/p pre-operative radiation therapy 20
Case Study: Gross Skin Muscle Potentially viable tumor Grossly necrotic tumor 21
Case Study: Fluorescent Imaging TEXT Viable Tumor Necrosis Myxoid Tumor Muscle 22
Mouse vs. Human Trials Question: What fluorescence values will we see in mice if we use the human clinical trial dose and imaging time parameters?
Summary and Plan We have administered a novel, cathepsin activated fluorescent imagine probe to 6 patients with sarcoma No adverse pharmacologic events Able to image tumors, but with decreased overall signal intensity and tumor:normal ratio than in mice Probe serum half-life in humans same as in mice Revising the Protocol Change imaging time from minimum 24 h to 6 h -Approved by IRB Patients 7 and 8 scheduled in next 30 days Additional research site under consideration 28
Acknowledgements • Clinical research team • Brian Brigman • Will Eward • Diana Cardona • Dan Blazer • Paul Mosca • Joan Cahill • Erin O’Reilly • DCI Clinical Pharmacology Laboratory • Ivan Spasojevic • Duke BME • Jenna Mueller • Statistical Support • Bercedis Peterson • Kirsch Lab • David Kirsch • MelodiJavid • Jeff Mito • Kyle Cuneo • Nerissa Williams • MIT • MoungiBawendi • Linda Griffith • Lumicell Diagnostics • Jorge Ferrer • David Strasfeld • David Lee 29