Download
1 / 110

E N D
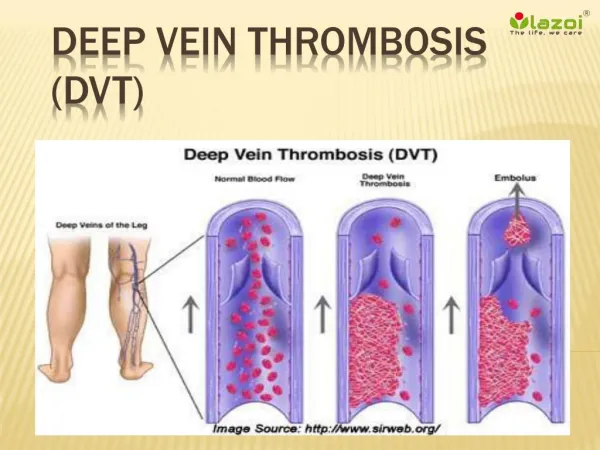
DIAGNOSIS AND MANAGEMENT OF ACUTE DEEP VEIN THROMBOSIS A joint consensus document from the European Society of Cardiology working groups of aorta and peripheral vascular diseases and pulmonary circulation and right ventricular function MUHAMAD RIZKI FADLAN Pembimbing dr,NoviKurnaisari, Sp.JP (k)
BACKGROUND Risk for first DVT seems to be slightly higher in men (1.3:1.1::male:female per 1000 person- years) The risk for recurrence of this disorder is higher in men than in women • Incidence of first DVT is 5 per 1000 person-years & PE 0.69/1000 personyrs. • The disorder is rare in children younger than 15 years, but its frequency increases withage. • Two-thirds of first-time episodes of deep vein thrombosis are caused by risk factors, including surgery, cancer, immobilization or admission for otherreasons. Risk for first DVT seems to be slightly higher in men (1.3:1.1::male:female per 1000 person- years) The risk for recurrence of this disorder is higher in men than in women
Patients with a scoreof 0 : lowrisk, 1–2 : intermediaterisk, ≥3 : highrisk
For the initial rule, patients with a score of 0–1 : lowrisk • 2–6 : intermediaterisk • ≥7 : highrisk; • For the dichotomisedrule, • score ≥4 likely to havePE • score≤4, unlikely to havePE
Patients with ascore <2 : lowrisk, 2–6 : intermediaterisk, ≥6 : highrisk.
Clinical features ofDVT Calf pain or tenderness, or both Swelling with pitting oedema Increased skin temperature and fever Superficial venous dilatation Cyanosis can occur with severe obstruction Less frequent manifestations of venous thrombosis include • Phlegmasia alba dolens, Phlegmasia cerulea dolens, and Venous gangrene.
Fibrin D-Dimermeasurement • Plasma D-Dimer is a degradation productof cross linked fibrin and its levels increase in plasma of patients with acuteVTE. • DD assay is highly sensitive(>98%) in acute DVT orPE • (cutoff value of 500mg/l) Hence, a DD levelbelow this value reasonably rules out acuteVTE.
Sensitivity is very high but specificity of fibrin for VTE is poor, because fibrin is produced in a wide variety of conditions such as cancer, inflammation, infection ornecrosis. • D-Dimer >500 mg/l has a poor positive predictive value for VTE. So it must be combined with clinical probability in orderto safely rule outVTE.
Venography was considered the diagnosticstandard for diagnosing DVT but it is invasive, costly and not devoid of risk. It is still used as surrogate end point inthrombo prophylactictrials.
Pulmonaryangiography Although gold standard for diagnosing PE, pulmonary angiography is difficult to interpret, frequent disagreement occurring even between expert readers, more often on the absence (17%) than on the presence of PE(8%).
Compression ultrasonography(CUS) • Lower limb compression venous USG, a noninvasive test with sensitivity of 97% & specificity of 98% for symptomatic proximal DVT.
The single well-validated diagnostic criterion for DVT on CUS is absence of full compressibility of the deep vein when applying pressure through the ultrasound probe.
Ventilation/perfusion lungscintigraphy • Perfusion lung scintigraphy is a noninvasive technique allowing the visualisation of pulmonary perfusion through IV albumin macroaggregates labelled by technetium 99. These are trapped in pulmonary capillary vessels and imaged by a gammacamera. • Pulmonary hypo-perfusion is not highly specific for an embolus, since any disease that narrows the airwaysor fills the alveoli with fluid will result in hypoxic pulmonary vasoconstriction.
A perfusion defect corresponding to a segment ora large part of a segment is more specific forPE. • The addition of ventilation scintigraphy(by xenon 133, krypton 81 or aerosolised technetium99) • further increases specificity, a so-calledmismatched defect (perfusion defect with normal ventilation) representing • PE.
lung scan results are classified into three categories: normal, high probability and nondiagnostic • Attribution of a lung scintigram to the high- probability category requires two or more mismatched segmental defects or, if only one is present, the addition of two large mismatched sub segmentaldefects
Spiral CTscan • Spiral CT scanning allows an adequatevisualisation of the pulmonary arteries up to segmental level.With sensitivity 70% & specificity of90%..
Multi-detector CT is highly sensitive, which allows both a thinner collimation (1–2mm collimation) and a better definition of thepicture. • CT angio has largely replaced ventilation perfusion scan as main imaging modality inPE • The probability of PE is very low in patients with a low or intermediate clinical probability, absence of proximal DVT and a negative spiralCT.
Echocardiography • Doppler echocardiography is not a diagnostictool, but in suspected PE it may play a role in risk stratification. • In 4% of patients, transthoracic echo allows direct visualisation of the clot in the right heart chambersor in the right main pulmonaryartery.
Echocardiographic manifestations of PE are acute increase in pulmonary arterial resistance and pulmonaryhypertension. • Signs : dilation of the right ventricle, hypokinesis, and in severe cases, paradoxical motion of the interventricularseptum. • In patients with shock, it is extremely effective for differential diagnosis with tamponade and cardiogenicshock.
Magnetic Resonance VenousImaging (MRVI) • Help in the imaging of more proximal venous disease. • Useful test for imaging iliac veins, IVC, calf vein & recurrent DVT and area where the use of duplex ultrasound islimited.
MassivePE • In highly unstable patients startthrombolytic treatment. • If patient is temporarily stabilised by vasopressive drugs, diagnosis is confirmed by either lung scan or spiralCT.
Recurrent deep veinthrombosis • Clinical assessment of recurrent ipsilateral DVT is hampered by the similarity between symptoms of post-thrombotic syndrome and acuteDVT. • Use of ultrasonography is limited because abnormalities in the proximal veins and comparison with previous USG resultsneeded.
Diagnosis of recurrent DVT requires the detection of a new non-compressible segment by USG. • If the result is nondiagnostic or negative, with high clinical probability, venography should be done.
Chronic thromboembolicpulmonary hypertension • Defined as a mean pulmonary artery pressure greater than 25 mm Hg that persists 6 months after diagnosis of pulmonaryembolism. • The disorder occurs in 2–4% of patients after acute pulmonary embolism and results in disabling dyspnoea, both at rest and with exertion.
Post-thrombotic syndrome of theleg • Post-thrombotic syndrome of the leg arises in 20-50% of patients with first proximal DVTwho has received standard treatment with anticoagulants. • PTS include chronic calf swelling withbrownish skin pigmentation and in extreme circumstances venous ulceration of theskin.
Risk factors are recurrence in theipsilateral leg and possibly proximalthrombosis. • In most people, the disorder arises within2 years.
Deep vein thrombosis of thearms • Symptoms include pain, oedema, and cyanosis. • Deep vein thrombosis of the arms arises as a complication of central venous catheters, or idiopathic (0·02 /1000 people peryear)
On clinical suspicion, compression CUS is the preferred diagnosticmethod. • If USG is inconclusive or negative despite a high clinical probability, venography should be done.
Treatment • Initialtreatment • Fixed-dose, weight adjusted, subcutaneous LMWH is treatment ofchoice. • Dose, 1mg/kg body weight twice daily or 2mg/kg body weight oncedaily. • Because of its shorter half-life, unfractionated heparin might be used in surgical patients with DVT in whom rapid reversal of anticoagulation is necessary.
Thrombolytic therapy • It should be reserved for patients with limb- threatening thrombosis • Given either systemically or via local catheter- directed infusion.
Vena cavafilters • In patients with proximalDVT • Vena cava filters are thrombogenic and double the recurrence risk. They used selectively in patients with • contraindications to anticoagulants, • recurrent PE despiteadequate anticoagulation, • chronic thromboembolicpulmonary hypertension.
Endovascular reconstruction • Recanalisation of occluded iliac veinis performedendovascularly. • Balloon dilatation is then performedand stent is placed across the dilated segment. • This is the first line therapy for iliac vein occlusions.
Long-termprevention • vitamin K antagonists started simultaneously with heparin (sameday) • The dose is titrated to achieve INR between2-3. • Heparin can be discontinued after 5–7 days, as long as the ratio is stable and is 2·0 orgreater.
Topic1 Ann Fam Med2007;5:63-73.
This journal summarizes the evidence regarding the efficacy of techniques for diagnosis of deep venous thrombosis(DVT) and pulmonaryembolism.
INTRODUCTION • The incidence of isolated DVT isaround 50 per 100,000person-years • 30% of patients with DVT develop symptomatic PE and another 40% have asymptomatic PE.
Article Review Process andData Abstraction • They reviewed 22 systematic reviews and36 primarystudies.
CLINICALPREDICTION RULES
Result • Results provide strong evidence to support the use of a clinical prediction rule for establishing the pretest probability ofdisease in a patient before more definitivetesting. • Use of a D-dimer assay with a clinical prediction rule has a very high negative predictivevalue.
The Wells prediction rule was most frequently evaluated in thesestudies