Download
1 / 48
510 likes | 892 Views
Neurosurgical Issues in Spina Bifida. Lori A. McBride, MD Children’s Hospital New Orleans. What does “Spina Bifida” mean?. Multiple related disorders Name refers to appearance on plain Xray: bifid (=split) spine

E N D
Neurosurgical Issues in Spina Bifida • Lori A. McBride, MD • Children’s Hospital New Orleans
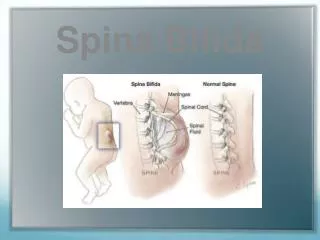
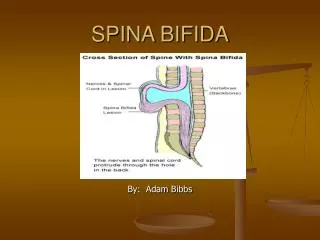
What does “Spina Bifida” mean? • Multiple related disorders • Name refers to appearance on plain Xray: bifid (=split) spine • All involve failure of the neural tube to disconnect from the skin, form a tube, and close correctly
What does “Spina Bifida” mean? • Some skin-covered and some not • If not skin-covered, associated with brain malformation (Chiari II)
Closure of Neural Tube 1. Sheet of ectoderm 2. Neural “groove” forms down center 3. Edges come together as a tube 4. Future spinal cord breaks away from skin
Glossary • Bifida / bifid = split in to 2 pieces • Myelo = spinal cord • Meningo = meninges (membranes around the brain and spinal cord) • Lipo / lipoma = fat • -cele / -coel = hole or defect
Types of Spina Bifida • Spina bifida aperta aka”open” • Myelomeningocele (MM) • Most common permanently disabling birth defect in US • Most common non-lethal CNS birth defect • Cord non-functional at and below lesion • Focus of today’s talk
Spina Bifida Aperta • Decreased incidence last 50 years • Incidence 3.2/10,000 births • Likely due to many factors: • Maternal nutrition • Folate • Prenatal diagnosis/selective termination
Types of Spina Bifida • Spina bifida occulta aka “closed” or “hidden” • BAD BAD BAD term as it now has 2 different meanings: • Skin covered lipomyelomeningocele, a type of tethered spinal cord • Insignificant bony abnormality
Lipomyelomeningocelefat + spinal cord + meninges +defect • AKA Spinal lipoma • Spinal cord is always stuck (tethered) in it and should be released • Skin is closed, but any layer beneath can be abnormal (cord, bones, muscle, fascia) and stuck to the lipoma • Often has “cutaneous stigmata” or abnormal skin overlying it • IQ typically normal, hydrocephalus rare
Spina Bifida Occulta (#2) • Absent spinous process only • No other abnormalities • Found in 10 to 30% of the population • Considered a “normal variant”
Myelomeningocele • Really 3 separate (but related) neurosurgical issues: • Spinal cord malformation (early and late issues) • Chiari II malformation • +/- Hydrocephalus
Chiari II Malformation • Multiple brain abnormalities including: • low-lying cerebellar vermis (“peg”) • medullary “kink” • low-lying elongated 4th ventricle • “beaked” tectum (midbrain) • low-lying venous sinuses • due to CSF leak during development?
Chiari II Malformation • Often assoc with hydrocephalus • May require surgery if symptoms of brainstem compression arise • Most remain asymptomatic
Hydrocephalus and Spina Bifida • 85% of MM patients have hydrocephalus • >90% in T-L region MM • 50% in sacral region MM
Worrisome Symptoms: Infancy • Death in the first 2 decades is usually caused by shunt malfunction or Chiari malformation • Shunt symptoms: progressive headache, nausea/vomiting, lethargy, or any symptom noted with prior malfunction • Chiari symptoms: breathing/swallowing problems, change in voice, headache
Worrisome Symptoms: Older Children • Scoliosis • Spasticity • Lower extremity changes • Shunt malfunction symptoms • Fewer Chiari symptoms
Spasticity • Increased muscle tone due to abnormal nerve input. Can show up as: • Tight muscles • Foot/leg deformity or asymmetry • Hip dislocation • Painful muscle spasms
Neurogenic Bladder • 80-90% of MM patients • Clean intermittent catheterization (CIC) has largely replaced diversion surgery • Almost 90% of patients have “social” continence
What is a “Tethered” Spinal Cord? • Spinal cord normally ends at T12-L1 level and hangs freely in the bony canal • Cord is tethered if it is scarred or stuck in the canal, esp at a lower level • As the baby grows, tension increases on the cord, causing damage • Only treatment is surgery
Symptoms of “Tethered” Spinal Cord • Progressive weakness • Ascending numbness • Gait Change • Progressive orthopedic deformity • scoliosis, in-turned foot, high arches, hammer toes, leg atrophy
Symptoms of “Tethered” Spinal Cord • Back pain (more common in older children/adults) • Change in bladder control/pattern (wet wet between caths, increase in UTI’s, etc)
MRI in Spina Bifida • MRI will always appear tethered (for life), so NOT helpful for ruling in or out tethered cord • Helps evaluate OTHER lesions such as syrinx, dermoid cyst, Chiari
What studies ARE helpful to evaluate for tethered cord? • Detailed history and serial neuro exams • usually make the diagnosis, but can be supplemented by: • Serial SSEP’s (SomatoSensory Evoked Potentials): accurate but painful test of spinal cord function • Serial Urodynamic studies to follow detrusor (bladder muscle) function
Shunt Malfunction • Can simulate ANY of the above symptoms due to CSF diversion down central canal of spinal cord (=syrinx) • Think of shunt especially if “tethering” is acute • Evaluate closure area on back for subQ fluid • Always check CT head before untethering surgery!
Shunts and Spina Bifida • ALWAYS • evaluate the shunt FIRST • for any clinical change!
Random Issues • (that I get asked about a lot)
Hydrocephalus Treament and Spina Bifida • Shunts are generally considered permanent, but MM patients have been reported to become shunt-independent • This likely happens more than we know as the patients have no outward signs
Endoscopic Third Ventriculostomy • An alternative treatment for hydrocephalus used to avoid a shunt • Results in infants are uniformly poor • Some success has been reported in converting older shunted patients to ETV, but there are no guarantees!
Spina Bifida Genetics • Definite genetic component • Does not follow strict “mendelian” genetics, so very difficult to predict accurately
Familial Risk of Spina Bifida • Spontaneous Risk: 0.05% • One Affected Sibling: 5% • Two Affected Siblings: 12-15% • Affected Mother: 3%
Intellect and Spina Bifida • IQ not as low as once thought • Made worse by multiple factors: • hydrocephalus • higher lesion level • shunt infection • half-hearted treatment of hydrocephalus
Intellect and Spina Bifida • Better verbal IQ than performance IQ, esp math and visual/spatial perception • Famous for “Cocktail Party Chatter” but poor school performance • McClone reported (1990) below avg (but normal range) IQ. MM group fell farther behind with age • Newer studies imply MM without hydrocephalus may have normal IQ
MOMS Study • Started 2003, published Feb 2011 in NEJM • Surgeries performed at 3 centers only--CHOP, Vandy, UCSF • Children evaluated at 12 and 30 months for hydrocephalus, Chiari, motor level, walking, IQ, and others
MOMS Study-- Positive Outcomes • CSF Shunts • Prenatal 40% Postnatal 82% • Chiari II • Pre 64% Post 96% • Ambulatory without orthotics • Pre 42% Post 21%
MOMS Study--Negative Outcomes • Prematurity--avg 34.1wks in prenatal group, with 13% delivered at <30wks vs 37wks in postnatal • 1/5 prenatal had resp distress syndrome • Multiple pregnancy complications • 1/3 prenatal had thin uterine wall • More tethered cords (8% pre vs 1% post) • 2 prenatal deaths post op
Prenatal Closure of MM • Open abdominal wall and uterus • Position baby so that MM shows through window • Close MM • Close uterine wall • Pray!