Download
1 / 15
150 likes | 390 Views
Clinical Predictors of Pneumonia Among Children with Wheeze. Dr. Simon Benson GP Specialist Trainee. Introduction. Diagnosis of pneumonia in children with wheeze is difficult Limited data exists regarding predictors of pneumonia among children with wheeze

E N D
Clinical Predictors of Pneumonia Among Children with Wheeze Dr. Simon Benson GP Specialist Trainee
Introduction • Diagnosis of pneumonia in children with wheeze is difficult • Limited data exists regarding predictors of pneumonia among children with wheeze • Asthma and bronchiolitis are two of the commonest presentations to ED – difficult to distinguish these from those with pneumonia • Result is unnecessary chest radiographs (CXR)
Objectives • Investigate value of historical features andclinical findings in patients with wheeze on examination for whom a CXR was ordered • To develop a clinical decision rule for the use of CXR in this patient population
Study Design • Prospective cohort • Inclusion criteria • Children less than 21 years old • Wheezing on examination • CXR performed • Attending ED between 01/10/2006 and 30/10/2007 • Attending Children’s Hospital Boston, Boston MA, USA
Study Design • Exclusion criteria • Chronic respiratory illnesses (eg cystic fibrosis) • Illnesses that may predispose to pneumonia (congenital heart disease, sickle cell anaemia, immunosuppression, malignancy) • Other potential causes for wheeze elicited on history (eg trauma or foreign body aspiration)
Study Design • Doctors were orientated to study and reminded monthly • Questionnaire completed prior to CXR request • Specific historical features (eg cough, fever, wheeze, chest pain) • Examination findings • Level of respiratory distress • Reason for requesting CXR • Response to inhaled bronchodilators • Some basic observations were also recorded (Temp, RR, oxygen saturations)
Study Design • CXRs were read by two blinded radiographers • Asked to decide whether normal or abnormal • If abnormal were findings more or less likely to be caused by atelectasis or pneumonia • If they failed to agree – original report used as final diagnosis. • Control group used to assess sample bias was drawn from all patients receiving CXR for first 3 days of each month
Results • 540 patients included initially • 14 excluded due to chronic illness • 526 patients included in the study • 59% were male • Median age 1.9 years (IQ range 0.7-4.5) • 47% of patients had a past medical history of wheeze • 15% received antibiotics • 5% patients were diagnosed with pneumonia
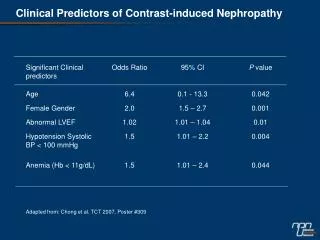
Results • 81% patients with pneumonia had a history of fever • 73% patients with pneumonia had temp > 38.0 in ED • Compared to 38% without • Those patients presenting with a fever or history of a fever had were twice as likely to have pneumonia but this increased to nearly five times more likely if a temperature of over 39.0 was recorded in ED • All these results are significant
Conclusion • Radiographic pneumonia in children with wheeze is uncommon • Historical and clinical features may be used to determine the suitability of CXR in a patient presenting with wheeze • Routine use of CXR for children with wheezing but without fever should be discouraged.
Discussion • Includes children with asthma • Supports previous work • Included children up to age 21 – extrapolation by age group is very difficult – anatomy and physiology vastly different at each end of spectrum • Busy emergency department – how many lost patients (estimated at 39% of all eligible patients) • CXR ordered at discretion of the doctor not according to predefined criteria (introduces selection bias)
Discussion • Did not include outcomes for children with wheeze who did not have a CXR – can not generalise to all children with wheeze • Likely overestimation of rate of pneumonia in wheeze • Viral versus bacterial • Some disagreement between radiologists did occur – could have used WHO guidelines for radiographic diagnosis of pneumonia but this may not apply with wheezing because of the presence of atelectasis
Final Thoughts • Generally good paper • Generally good quality and reliable results • Enables a solid evidence based conclusion to be drawn that is: • Routine use of CXR for children with wheezing but without fever should be discouraged.