Download
1 / 35
350 likes | 599 Views
Female Genitourinary System. External : Vulva aka “perineum”; from mons pubis to anus. Mons pubis = fat pad located over symphysis pubis. Labia majora –outer folds of skin within mons pubis. Labia minora –2 folds inside labia majora.

E N D
Female Genitourinary System • External: Vulva aka “perineum”; from mons pubis to anus. • Mons pubis = fat pad located over symphysis pubis. • Labia majora –outer folds of skin within mons pubis. • Labia minora –2 folds inside labia majora. • Clitoris anterior to labia minora; func.similar to penis; contains erectile tissue. • Either side of urethra: Skene’s glands > secretions > keep vaginal area moist. • Either side of vagina: Bartholin’s glands >secrete mucous during intercourse. Visible with infection.
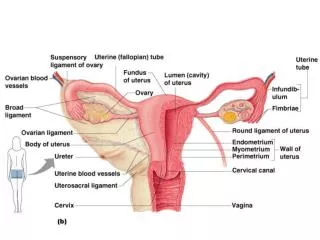
Cervix: neck of uterus. “Os” opening Never pregnant: small, round os. + vagina delivery: slit-like Made of smooth muscle & connective tissue [2 types of epithelium: squamous & columnar]. Cells tested during Pap & analyzed for abnormalities. Func: allows sperm to enter & menstrual flow to exit. Uterus: upside down hollow pear-shaped muscle; Lies in pelvic cavity; tilts forward “anteverted”. Holds & protects growing fetus. 3 layers: endometrium, myometrium, perimetrium. Fundus: top portion; Endometriumsheds w.menses.
Ovaries: small, oval-shaped organs [~ 2 cm by 3 cm by 1 cm] Influenced by FSH & LH - “gonadotropic hormones; causes ovum to grow & mature monthly. Produced by anterior pituitary gland. Ovaries connect to uterus by fallopian tube. Develop & release ova & produce hormones: estrogen, progesterone & testosterone [small amts.in females]. Ova released from ovary, enters fallopian tube, travels to uterus.
Puberty: Anterior pituitary releases FSH & LH > androgens & estrogen [both females & males] > secondary sex characteristics. • Reproductive age begins here; girls get menses earlier now - d/t PNV & better diets . • Age 10-12 not uncommon. Gametogenesis: production of specialized sex cells [gametes]. Male and Female. By age 22, ~ 300,000 eggs remain; by menopause, none remain. • Cyclic monthly release of eggs > “menses” or they are absorbed.
## of chromosomes in nucleus of gametes halved from 46 to 23 ( meiosis) [22 autosomes & 1 sex chromosome – either X or Y]. • In females occurs before ovulation each month & in males occurs before puberty. • Ovum have X chromosome & sperm have either X or Y. Male determines sex: XX=female; XY = male.
Male Genitourinary System External: penis & scrotum. • Male reproductive organ = penis. • Shaft made of vascular erectile tissue. • “Glans” tip/end of penis; covered by thin skin aka “foreskin”. • Circumcision removes foreskin. Urethral “meatus” –slit-like opening located @ tip. Leads to tube “urethra” that reaches up to bladder. Func: reproduction & urination. • Scrotum [thin walled sac] posterior & encloses testes. • Surface > folds of skin aka “rugae” =normal. Protects testes, epididymis, & vas deferens.
Internal Genitalia: scrotal sac divided in 2. • One testis on each side. Oval shaped. • Produce sperm & testosterone. • Suspended by spermatic cords. • Spermatic cord: blood vessels, lymphatic vessels, nerves, cremasteric muscle [very sensitive to temp.changes - controls rise & relaxation of scrotum in hot & cold weather] • Keeps temp.cooler than normal
Epididymis: lies over testes. Allows spermatozoa to mature. • Vas deferens [part of epididymis] allows sperm to exit. • Semen = sperm & secretions from glands [Cowper’s/prostate/bulbourethral]
Breasts • Pair of mammary glands • 1] production & storage of milk = “lactation” • 2] sexual stimulation. Male breasts = no func. • Lie over pectoral muscles of anterior chest wall • Extend from 2nd to 6th rib & from sternum to midaxillary line. • Male & female breasts similar til puberty. • Estrogen & progesterone, released by ovaries, causes growth of breast tissue @ puberty. • Divided into 4 quadrants
Breast skin smooth; color varies with skin tone. • Nipple centrally located; microscopic openings [excretory ducts]>allow milk to pass [lactation] • Areola darkened, circular area around nipple; has raised nodules [sebaceous glands] “Montgomery tubercles” - oily substance cleans nipple. • Areola enlarges & darkens; does not return to normal size & color > preg. • Color depends on person’s skin tone.
Internal Structure: 3 types of tissue 1] Glandular: functional >> breast milk prod. • Each breast 15-20 lobes • Each lobe contain alveoli > made up of acinar cells. • Alveoli secrete milk into lactiferous ducts where it passes > lactiferous sinuses [milk reservoirs] & released thru excretory ducts > nipple. • 2] fat • 3] muscle
Amount of breast tissue affected by: Menses: Engorgement 3-5 days < menses. Breasts ^ in size, density, sensitivity, & nodularity. Menopause: breast tissue becomes less dense & decrease in size [d/t lack of estrogen]. Breast exam best done 1 week > menses. Pregnancy/Lactation: fuller & firmer; areola darkens; nipples erect. Produce colostrum & breast milk.
Review Of Menses: • Menstrual Cycle has 2 phases: uterine & ovarian. • Uterine Phase: 1] menses 2] proliferative 3] secretory • Menses: ~5 days [shedding of uterine lining] • Proliferative: thickening of endometrium; day 5-14 • Secretory: day 14-28; ↑ progesterone makes lining rich in nutrients. If no fertilization: progesterone & estrogen fall; lining degenerates. Menses 2-3days later. • Menstrual flow: blood, mucous, frag.of endometrial tissue, & unfertilized ovum.
. Ovulatory Phase: 1] follicular 2] ovulation 3] luteal • Follicular: Influenced by FSH, one ovum grows & is surrounded by follicle. Mature graafian follicle moves to edge of ovary to release egg. • Ovulation: occurs > LH surge; follicle ruptures & ovum released; waits to be fertilized in fallop.tube • Luteal: if not fert.,ovum & corpus luteum shrink. If fert.,corpus luteum stays til ~10 -12 wks. Produces progesterone to sustain fetus/pregnancy until placenta develops
Basic Concepts • Genetic information stored on tightly coiled strands of dexoxyribonicleic acid (DNA) called chromosomes. • Chromosomes composed of DNA, histone proteins [+ charge] & non-histone proteins. Bind very tightly. • Chromosomes contain thousands of genes; smallest units of heredity information • Cells express only some of their genes. Genes expressed determine function of cell. If genes have incorrect information, defects follow.
Mutations result from changes in DNA sequences. • Normal number of chromosomes = 46. • 22 pairs of autosomes & 1 pair of sex chromosomes = 23. “Meiosis” • Female: meiosis: occurs before ovulation & in males occurs before puberty
Human Genome Project (1990-2003); research on genetic mutations & inherited diseases. • Identified ~ 30,000 genes in humans • Pictorial analysis (karotype) can be performed on any tissue. (phenotype = what’s expressed) • Genetic disorder can be classified as either congenital or hereditary • Congenital : Present @ birth. Occurs @ conception. Can involve abnormal chromosome #, structure, or multifactorial (genes & environment ) • Ex. Vent.septal defect, hypospadius, cleft lip & palate. • Hereditary: Predetermined by family hx. Transferred from parent to child: Sickle cell disease, & cystic fibrosis.
Some Currently Available DNA-Based Gene Tests • Amyotrophic lateral sclerosis (ALS; Lou Gehrig's Disease; progressive motor function loss leading to paralysis & death) • Alzheimer's disease* (APOE; late-onset variety of senile dementia) • Ataxia telangiectasia (AT; progressive brain disorder resulting in loss of muscle control & cancers) • Congenital adrenal hyperplasia (CAH; hormone deficiency; ambiguous genitalia & male pseudo-hermaphroditism) • Cystic fibrosis (CF; disease of lung & pancreas results in thick mucous accumulations; chronic infections)
Cont. • Duchenne muscular dystrophy/Becker muscular dystrophy (DMD; severe to mild muscle wasting, deterioration, weakness) • Dystonia (DYT; muscle rigidity, repetitive twisting movements) • Fanconi anemia, group C (FA; anemia, leukemia, skeletal deformities) • Factor V-Leiden (FVL; blood-clotting disorder) • Fragile X syndrome (FRAX; leading cause of inherited mental retardation) • Gaucher disease (GD; enlarged liver & spleen, bone degeneration)
Cont. • Inherited breast and ovarian cancer* (BRCA 1 and 2; early-onset tumors of breasts/ovaries) • Hereditary nonpolyposis colon cancer* (CA; early-onset tumors of colon. • Hemophilia A and B (HEMA & HEMB; bleeding disorders) • Hereditary Hemochromatosis (HFE; ^^ iron storage disorder) • Huntington's disease (HD; usually midlife onset; progressive, lethal, degenerative neurological disease)
Cont. • Myotonic dystrophy (MD; progressive muscle weakness; most common form of adult muscular dystrophy) • Neurofibromatosis type 1 (NF1; multiple benign nervous system tumors that can be disfiguring; cancers) • Tay-Sachs Disease (TS; fatal neurological disease of early childhood; seizures, paralysis) • Phenylketonuria (PKU; progressive mental retardation d/t missing enzyme; corrected by diet) • Adult Polycystic Kidney Disease (APKD; kidney failure & liver disease)
Cont. • Prader Willi/Angelman syndromes (PW/A; decreased motor skills, cognitive impairment, early death) • Sickle cell disease ( blood cell disorder; chronic pain and infections) • Spinocerebellar ataxia, type 1 (SCA1; involuntary muscle movements, reflex disorders, explosive speech) • Spinal muscular atrophy (SMA; severe, usually lethal progressive muscle-wasting disorder in children) • Thalassemias (anemias - reduced RBC levels)
Mendel’s laws: [1866] Principles of dominance • a. Genes not equal in strength • b. Stronger gene produces an observable trait; called dominant • c. Weaker gene; trait not seen; called recessive. Ex. brown eye color dominant over blue. • F1 generation always dominant • F2 generation produces both dominant & recessive traits
Principle of segregation • Paired chromosomes that contain genes from both parents separate during meiosis. Principle of independent assortment : • Pair of one set of genes distributed in gametes in random fashion unrelated to other pairs; in other words… • Chance determines whether maternal or paternal gene travels to specific gamete.
How can children from the same parents look so different? • Father's chromosomes >> his mother & father, • Mother's “” >> her mother & father. • To make sperm cell, ½ of genetic material is contributed. Which half? • When sperm cells form, father's body randomlychooses genes from two halves of father's chromosomes. • So, every sperm cell contains random mix of father's parents' genes. • Same thing occurs when forming eggs. Therefore, • each child that a couple produces is random mix of the 4 grandparents' genes.
Categories of Genetic Disorders Trait determined by 2 genes: one from each parent. Autosomal-dominant: abnormal gene on autosome. • require single copy of gene to be affected. One parent with disease for child to inherit disease. • Bad gene dominates good gene. • No "carrier“; everyone with genetic error gets disease. • Inherited thru non-sex chromosomes, pairs 1-22. • Each preg. 50/50 chance of having disease. • Examples: Neurofibromatosis; adult Polycystic kidneys; Huntington’s chorea; Marfan syndrome; breast, ovarian, & colon CA .
Autosomal Recessive: 2 abnormal genes to have disease. If 4 children produced & both parents carriers: STATISTICAL expectation: • 1 child: 2 normal chromosomes (normal) • 2 children: 1 normal & 1 abnormal chromosome (carriers, no disease) • 1 child: 2 abnormal chromosomes (+ disease) EACH child: 1 in 4 chance inheriting disorder & 50:50 chancebeing carrier. • Examples: Cystic fibrosis; sickle cell; Albinism; Tay-Sachs, tendency for venous thrombosis.
X-linked Inheritance: affects genes on X chromosome • X-linked recessive: No father to son transmission. • Males with X-linked disorder always give X chromosome to daughters. Daughters are carriers. • X-linked recessive genes expressed in females if 2 copies of gene (on each X chromosome). • Y chromosome has no genes. • In males, need only 1 copy of X-linked recessive gene for disorder to be expressed. Dominant in expression. • Males never carriers. • Examples: Hemophilia A; color blindness; Duchenne Muscular Dystrophy; Fragile X-linked mental retardation [~290 conditions exist]
X-linked dominant:rare. • Trait never passed from father to son. • All daughters of an affected male and normal female affected. All sons of an affected male and normal female are normal. • Males receive gene from mother; usually more severely affected than females. • Trait may be lethal in males. No carriers. • Examples: Coffin-Lowry syndrome & Familial rickets.
Chromosomal Deviations – Congenital • Deviation: either in # or structure of chromosome. • Structural defect can be d/t loss, addition, rearrangement of genes on chromosome or exchange of genes between chromosomes. Occurs during meiosis. • Deviations in # of chromosomes involve either gain or loss of entire chromosome during cell division. • Monosomy – lacks chromosome; incompatible w. life. Ex. Turner’s syndrome (one X) • Trisomy – extra chromosome
Cont. • Most common chromosomal disorder: Trisomy 21 aka Down’s Syndrome [95%] Extra chromosome = # 21. Trisomy 13; lower survival rate. • Nondisjunction: pair chromosomes don’t separate [Down’s] • Translocation: 2 or more chromosomes rearrange during meiosis. Too much/too little chromosomal material is received. Assoc. w. advanced maternal age [AMA]
Multifactorial Inheritance Disorders • genes & environment interact to produce (often) “Isolated” birth defect. • Can be mild to severe • no inheritance pattern but higher risk of recurrence observed in certain families. • Examples: risk for spina bifida ↓ with ↑ levels of folic acid in prenatal period. • Rate of HD ^ in moms with hx IDDM. • ^ FAS with ^ maternal alcohol intake. • ^ rate cleft lip/palate (in-breeding occurs) • Environmental risks include nutrition, diseases.
Detection of Genetic Disorders Preconception Screening Family Hx: determine disease & birth defect patterns. Take thorough family hx – photos. Prenatal Testing> 40 years recommended • Carrier testing -certain ethnic groups • ^ incidence diseases: Tay-Sachs, Sickle cell, Cystic Fibrosis Statistics: Risk for Trisomy 21 [Down’s] • Age 20-24 = 1/1400 births • Age 35 = 1/400; Age 40 = 1/100 • Age 45 = 1/25; Age 49 = 1/12
Post Delivery: • Biochemical Tests: PKU [NYS mandate]; tests ~ 50 genetic and congenital disorders {CF, sickle cell, PKU, congenital hypothyroidism} • Newborn Hearing Screen - congenital hearing loss • Cytologic Studies: DNA studies [karotype] • Dermatoglyphics: study of hand; simian crease in Down syndrome • Role of Nurse: offer support & allow to verbalize feelings; don’t offer “stories” of other pts. Don’t offer false hope; OK to verify feelings. • Ethical dilemma's may exist. • Non-judgmental approach.