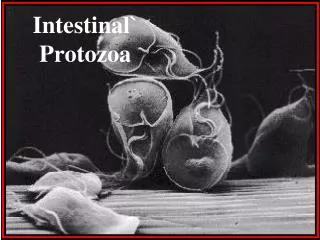
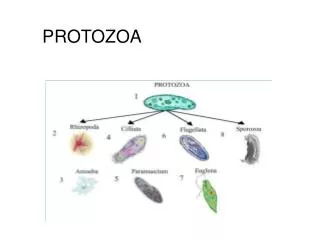
Intestinal protozoa
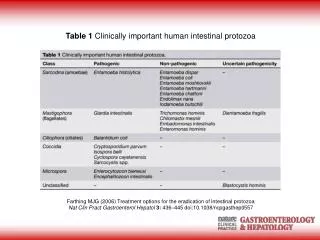
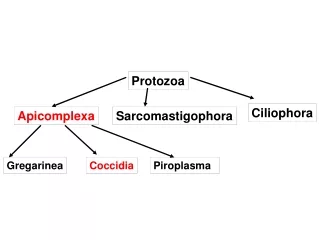
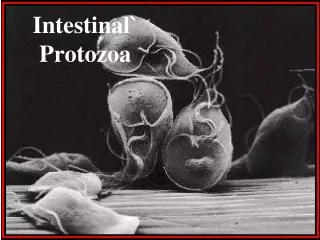
Intestinal protozoa. Amoeba: Entamoeba histolytica Flagellates: Giardia lamblia Coccidians: Toxoplasma gondii, Cryptosporidium parvum. 1. Protozoa colonize and infect the oro-pharynx, duodenum and colon 2. The organisms are transmitted by the fecal-oral route (food/water)

Intestinal protozoa
E N D
Presentation Transcript
Intestinal protozoa Amoeba: Entamoeba histolytica Flagellates: Giardia lamblia Coccidians: Toxoplasma gondii, Cryptosporidium parvum 1. Protozoa colonize and infect the oro-pharynx, duodenum and colon 2. The organisms are transmitted by the fecal-oral route (food/water) 3. Outbreaks of diarrhea and dysentery are especially problematic in daycare centers 4. The cyst forms of protozoa are resistant to chlorine and ozone and can become important when the municipal water supply is overburdened with these organisms—esp. farming communities Read Vela Chapter 7
Entamoeba histolytica Primitive unicellular micro-organisms Life cycle divided into two stages trophozoite—actively motile feeding stage—food and human blood cells when environmental conditions are favorable cyst—dormant, highly resistant, infectious stage when temperature or moisture levels drop Replication involves simple binary fission of trophozoite or division to produce numerous infectious trophozoites in a mature cyst. Motility—extension of a pseudopod (false-foot) and then drawing up the rest of the cell to meet the pseudopod in a “snail like” movement.
E. histolytica life cycle Encounter—fecal-oral route patients with diarrhea excrete the trophozoite form which is killed by drying in the environment or by the acidity of the stomach asymptomatic patients excrete infectious cysts that are resistant to drying and acid 1. Ingestion of cysts 2. Passage of cysts through the stomach where gastric acid stimulates the release of the infectious trophozoites from the cysts 3. Trophozoites move to the duodenum where they divide 4. Trophozoites travels to the colon where they attach to colonic epithelial cells 5. After attachment they produce a cytotoxin that kills epithelial cells so they can gain access to deeper tissues 6. Continue to divide in colon where amoeba/cysts are excreted in stool OR 7. Trophozoites invade the deeper mucousa and enter the peritoneal cavity 8. Trophozoites are carried in the circulation to the liver but can also be carried to the lungs, brain and heart
Epidemiology of E. histolytica Worldwide distribution—especially prevalent in warmer climates but also endemic cases found in cold areas (ie. Alaska, Canada) Many infected individuals can be asymptomatic and serve as reservoirs Ffor disease Carrier passes cysts that contaminate water supply and food—esp children in daycare centers Flies, ants and cockroaches can also serve as vectors for the spread of cysts Sewage containing cysts can contaminate municipal water supply wells and springs. Use of human feces as fertilizer can contribute to the spread Prevalence of infection in U.S. is 2-5% in warmer countries 15-50%
Clinical diseases of E. histolytica Amoebic dysentery!!! Related to the destruction of the colonic epithelial cells by the organism. Flask shaped ulcerations of the intestinal mucousa with inflammation Secondary bacterial infection symptoms: abdominal pain, cramping passage of numerous watery and bloody stools If untreated patients can die of dehydration Amoeba can invade deeper tissues and enter the blood circulatory system where they especially infect the liver as trophozoites are re- moved from blood as they enter the liver. abscess formation in the liver is common pain in the liver and elevation of the diaphragm
Treatment and prevention of E. histolytica Metronidazole—penetrates deeper tissues and destroys amoeba present in liver, brain, lungs etc. the organism’s metabolism converts the drug into its lethal form A second drug is used to eradicate the amoeba present in the intestinal lumen (paromomycin) Prevention: When traveling to areas where E. histolytica is epidemic or endemic AVOID drinking water ALSO ice cubes filter and boil water thoroughly wash unpeeled fruits and raw vegetables
Giardia lamblia trophozoite Giardia attached to intestinal microvilli by sucking disks Upon detaching clear impressions from the Sucking disks are left on the surface of the microvilli G. lamblia is a flagellate and moves by lashing its flagella that moves organism through fluid environments. G. lamblia attaches to the intestinal villi of duodenum via an adhesive disk Cysts are resistant to the amounts of chlorine put in municipal water systems (2 parts per million) therefore water systems should ALSO filtrate water
G. lamblia life cycle • 1. Infection initiated by the ingestion of infectious cysts (only 10 are • required for infection • 2. Acid in the stomach stimulates the release of trophozoites from the • cyst • 3. Trophozoites are released in the duodenum and jejunum (upper part • of small intestines) where they multiply by binary fission • 4. Trophozoites attach to the intestinal villi by means of a sucking disk • Trophozoites can develop into cysts for survival outside of the host • Trophozoites cause an explosive diarrhea such that cysts are released • into the environment • Trophozoites remain in the G-I tract and almost never found • elsewhere in the body.
Epidemiology of G. lamblia G. lamblia found everywhere in the world Often found in streams, lakes mountain resorts—reservoir animals such as beavers and muskrats perpetuate the infectious cycle Approximately 50% of infected humans are asymptomatic and are important carriers of disease Giardiasis is acquired through the consumption of inadequately treated water ingestion of uncooked vegetables and fruits person-person spread (esp. daycare centers, families with infected children) Giardia can be maintained in the municipal water supply, unless water treatment plant uses filtration AND chemicals to eradicate the protozoa
Clinical diseases of G. lamblia Symptomatic disease ranges from mild diarrhea to severe dysentery The incubation period before symptomatic disease is approx. 10 days The onset of disease is sudden and consists of foul-smelling watery diarrhea (seldom bloody) abdominal cramping flatulence Spontaneous recovery occurs in 2 weeks HOWEVER Chronic disease with several relapses may occur.
Clinical diagnosis of G. lamblia With the onset of diarrhea the patient’s stool are examined for trophozoites and cysts. Giardia may appear in stool on a given day and not be present on the following day one stool sample over a period of three days should be examined before making a negative diagnosis. Samples can be collected through duodenal aspiration or via biopsy of upper small intestines.
Treatment and prevention of G. lamblia Eradicate Giardia from BOTH asymptomatic carriers and diseased patients. Campers/travelers should boil AND filter water taken from lakes and streams AND from municipal water in areas where disease is endemic Municipal water supplies should maintain functioning filtration Systems since the cysts are resistant to chlorine and ozone treatment
Coccidia—Crytosporidium and Toxoplasma Reproduce by sexual and asexual reproduction Most coccidiae have multiple hosts C. parvum found in farm animals/ reptiles and fish where they reproduce sexually they reproduce asexually in humans. T. gondii found in herbivores, birds and carnivores (sexual) and humans (asexual) cats are especially important carriers of disease Hard to eradicate because these protozoa are zoonotic