Download
1 / 56
600 likes | 993 Views
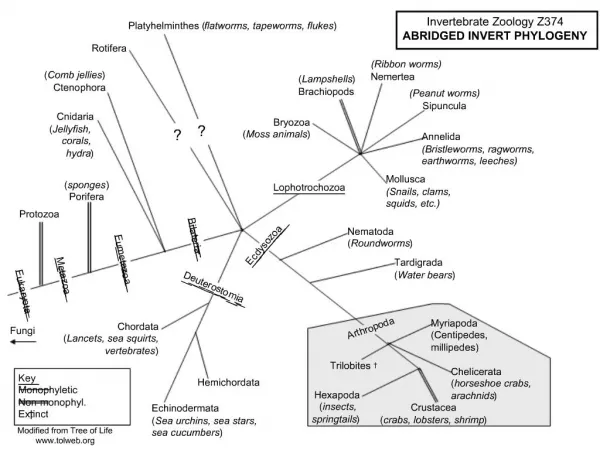
Protozoa. General Properties of protozoa Protozoa are one-celled animals with full vital functions. They may be freeliving or parasitic. Protozoa are minute parasites and can only be visualized under the microscope. Basic structure.

E N D
General Properties of protozoa • Protozoa are one-celled animals with full vital functions. • They may be freeliving or parasitic. • Protozoa are minute parasites and can only be visualized under the microscope.
Basic structure • Protozoa, the whole body consists of a singular cell. A protozoan cell is composed of : • 1)plasma membrane • 2)cytoplasm : a. ectoplasm(外质) b. endoplasm(内质) • 3)nucleus
Life cycle patterns • One-host form (direct) • One stage form – Trophozoite • Two stage form – Trophozoite & Cyst • Two-host form (indirect) • Mammals --- mammals • Mammals --- insect vectors
Locomotion(运动): • flagella(鞭毛) • cilia(纤毛) • pseudopodia(伪足).
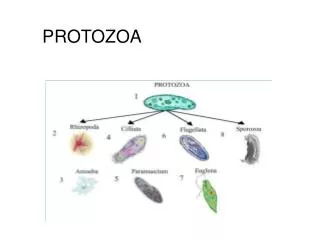
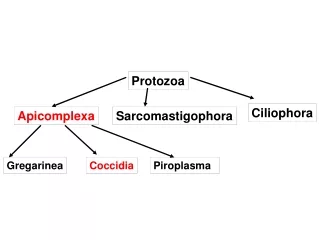
Pathologic characteristics of protozoa • 1. Multiplication (增殖) • 2. Diffusion (disperse ) • 3. Opportunistic pathogen (机会致病) • Classification of protozoa: • According their locomotion organelles, protozoa can be divided into four groups: Amoebae, flagellates, ciliates and sporozoan.
Ecological Niches in the Human Body: • 1. Skin: Leishmania • 2. Eye: Acanthamoeba • 3. Mouth: Amoebae and flagellates • (usually non-pathogenic) • 4.Gut: Giardia, Entamoeba (and invasion to liver), Cryptosporidium, Isospora, Balantidium • 5. Genitourinary Tract: Trichomonas
Ecological Niches in the Human Body: • 6. Bloodstream: Plasmodium, • Trypanosoma • 7. Spleen: Leishmania • 8. Liver: Leishmania, Entamoeba • 9. Muscle: Trypanosoma cruzi • 10. central nervous system: Trypanosoma, Naegleria, Toxoplasma, Plasmodium
Medical Protozoa • Pathogenic • Opportunistic parasite • Not normally pathogens • Become pathogenic due to impairment of host resistance • Clinical importance of the AIDS epidemic • Opportunistic parasites • An infection by a microorganism that normally does not cause disease but becomes pathogenic when the body's immune system is impaired and unable to fight off infection
Pathogenic Intestinal Amoeba Entamoeba histolytica 溶组织内阿米巴
Epidemiology • 4th leading cause of death from parasitic diseases worldwide • Organism# of deaths/yr# infected • Entamoeba ~75,000 ~300 million • Ascaris ~200,000 ~480 million • Schistosoma ~750,000 ~200 million • Plasmodium 2-3 million ~500 million • (Malaria) • Amoebiasis is not restricted to the tropics and subtropics, it also occurs in temperate and even in arctic and antarctic zones
granular endoplasm ectoplasm Entamoeba histolytica
Morphology • Trophozoite • Size: 10-40 m • Shape: ovoid with pseudopodium • Basic structure: cytoplasm, vesicular nucleus (chromatin granules, nuclear membrane, karyosome)
E. histolytica trophozoite Ingested RBC endoplasm Nucleus with central karyosome and fine regular granules(peripheral chromatin granules), evenly distributed around the nuclear membrane Ectoplasm,Pseudopod E. histolyticatrophozoite
E. histolytica Stages - TROPHOZOITES • Cause amoebiasis (damage tissue) • Spread throughout the body • Rarely transmit the infection to others • Labile in liquid stools or tissue, and • must be rapidly found or preserved (quick fixation & cold storage) for Dx
Two microscopically indistinguishable Entamoeba • E. histolytica • invades tissues • should always be treated, even in asx patients • E. dispar • is non-pathogenic, even in AIDS • should not be treated
E.histolytic cyst (schematic diagram) • Spherical or round in shape, 10-20um in diameter, cyst wall • 1-2 nuclei (immature cyst); 4 nuclei (mature cyst-infective stage). • Glycogen vacuole food reservoir (brownish-yellow,iodine stained) • chromatoid bodies with blunt, rounded ends in immature(young) cyst
E.histolytic cyst (schematic diagram) 4 ring-like nucleiwith finely divided peripheral chromatin , glycogen vacuole and chromatoid bodies disappear Cyst wall and round shape Mature E. histolyticaCyst
E. histolytica Stages - CYSTS • Infective Stage for humans • The stage of discharge • Diagnostic Stage in formed stools • Resistant to external surroundings
Mode of transmission • Humans acquire E. histolytica by: • Ingestingcysts (4 nuclei mature) in fecally contaminated food or drink • Rarely by directly inoculatingtrophozoites into colon or other sites (anal sex?) • Fecal-Oral transmission (hand to mouth)
Life cycle • The basic generation-cycle: cyst –trophozoites – cyst • Trophozoites may invade intestine and spread • Infective cysts and trophozoites pass in feces
Life Cycle • 1 infective stage: mature cyst • 2 access: mouth • 3 ecological niches: large intestine; liver, lung and other organs. • 4 pathogenic stage: trophozoite • 5 diagnostic stage: cyst; trophozoites
Pathogenesis • Pathogenic factor • Virulence • Species: • E.histolytica (pathogenic species) • E.dispar (non-pathogenic species) • Immunity of host • Bacteria flora菌丛
Clinical Classification of Amebiasis(World Health Organization) • Asymptomatic (intestinal) "Cyst Passers” • Symptomatic Infection: • Intestinal Amebiasis: (dysentery, colitis) • Acute Dysenteric (dysentery) • Chronic Non-Dysenteric (“self-cured”) • Extra-Intestinal Amebiasis: • Amebic Liver Abscess (ALA) • Amebic Pulmonary Abscess • Other sites (brain, skin, GU,)
Clinical classification • Asymptomatic infection (carrier) >90% (E. dispar?) • Symptomatic cases <10% • 8-10% dysentery, colitis, etc • 2% invasive amoebiasis • 0.1% deaths
Acute Dysenteric Amebiasis • Symptoms: • Bloody mucoid diarrhea • RBCs and few WBCs in stools • Abdominalpain • weight loss • Bloating(胃气涨), tenesmus(里急后重) and cramps (痉挛)
Acute Dysenteric Amebiasis • Signs: • Fever (33%) • Tender (enlarged) liver • Stools positive for trophozoites +/- WBC • NOT cysts in loose stools
Clinical manifestation • Pinpoint lesion on mucous membrane • Flask-shaped crateriform (volcano)ulcers
Chronic Non-Dysenteric Amebiasis • “self-cured” carrier state • Usually for 1 year, 37% symptomatic >5 years • Intermittent diarrhea, mucus stool, abdominal pain, flatulence and/or weight loss • E. histolytica trophs (rarely cysts) in stools • Positive serology and ulcerations on sigmoidoscopy or pathology test
Amebic Liver Abscess (ALA) Extra-Intestinal Amebiasis • Symptoms • History of dysentery (1 yr), wt loss, abdominal pain, chest or shoulder pain • Signs • fever, hepatomegaly 肝肿大 • Might find trophozoites in the aspirate • Skin inflammation
Extra-intestinal amoebiasis • Hepatic • (1) acute non-suppurative • (2) liver abscess: right upper quadrant pain, referred to the right shoulder. tender. • Pulmonary • Brain • Skin, perianal infection • Other extra-intestinal amoebiasis
An Amoebic Liver Abscess Being Aspirated. • Note the reddish brown color of the pus (‘anchovy-sauce’). This color is due to the breakdown of liver cells. Gross pathology of amebic abscess of liver. Tube of "chocolate" pus from abscess.
Diagnosis • Pathogenic diagnosis • Stool examination: • Direct Fecal Smear (trophs and cysts) • Fecal concentration and iodine dye techniques - (cysts) ZnSO4 or formalin-ether • Cultivation • DNA detection • Sigmoidoscopy • Serologic Tests (for chronic disease): ELISA, IHA (indirect hemagglutination) • Imaging: X-ray; CT
Treatment of Amebiasis • For invasive forms: metronidazole • For luminal forms: Iodoquinofonum, paromomycin, diloxanide • Do not treat asymptomatic intestinal E. dispar infection
Epidemiology • Cosmopolitan世界性的/worldwide • China: 3%~10%; Rural area>urban • Source of infection: carriers • Transmit route: water contamination • Insects: fly, cockroaches
Prevention & Control • Individual measures • Diagnosis and treatment of E. histolytica patients • no animal reservoirs (other than humans) are known • Safe drinking water (boiling or 0.22 µm filtration) • Cleaning of uncooked fruits and vegetables • Prevention of contamination of foods • Personal hygienic health education
cyst nucleus trophozoite E.h E.c
Question • 1.How to diagnose hepatic amebiasis? • 2.What are the transmission route of E. histolytica ? • 3.Who should be treated for amebic infection?
Giardia lamblia • It is a pathogen • of digestive tract.
Morphology of Giardia lamblia trophozoite looks like monkey face adhere to surface of intestinal cell Median body
Trophozoite of Giardia lamblia (under high power microscope, stained film)
Cyst of Giardia lamblia • Oval-shape,4 nuclei , • flagella and axostyle can be seen • Cyst wall