Download
1 / 44
440 likes | 460 Views
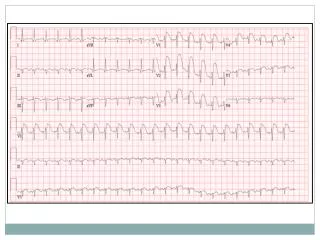
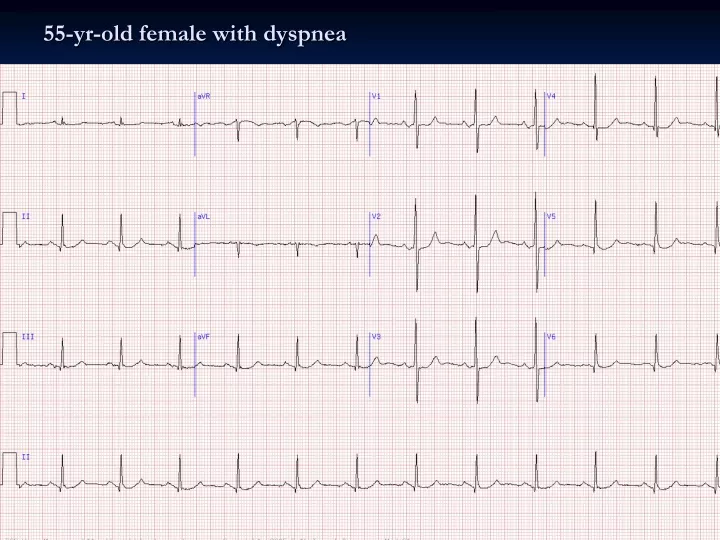
55-yr-old female with dyspnea. Interpretation: SR with LAA and RVH. Sinus rhythm at 70 bpm Vertical axis at 80-90 degrees Left atrial abnormality Biphasic P in V1 with broad negative component Broad P waves elsewhere Right ventricular hypertrophy Tall R in V1 R/S ratio in V1 > 1

E N D
Interpretation: SR with LAA and RVH • Sinus rhythm at 70 bpm • Vertical axis at 80-90 degrees • Left atrial abnormality • Biphasic P in V1 with broad negative component • Broad P waves elsewhere • Right ventricular hypertrophy • Tall R in V1 • R/S ratio in V1 > 1 • Rightward axis • Combination of LAA with RVH in dyspneic patient consistent with severe mitral stenosis (likely secondary to rheumatic heart disease)
Interpretation: SR with LBBB and AMI • Sinus rhythm at 70 bpm • Left axis deviation at -40 degrees • LBBB • Prior and possibly evolving myocardial infarction superimposed on LBBB • Prior MI is indicated by Q waves as part of a qR in I and V6 • Notching of the ascending limb of the S wave in the mid-left chest leads is also consistent with prior MI (Cabrera's sign) • Biphasic T waves in the mid-left chest leads raise consideration of evolving ischemia/MI • Anterior ST elevations non-diagnostic
ECG 101 – ECG Changes in Non-Cardiac Conditions Scott E. Ewing DO
Hyperkalemia • Classic hyperkalemia • Tall peaked / narrow T waves, i.e. “tenting” • PR prolongation • Also, underlying LVH (patient has renal disease with hypertension) • Potassium here was 9.6mEq/L • Not all tall positive T waves are “hyperacute”, term reserved for increased T wave positivity secondary to transmural ischemia • Note: QRS prolongation also seen with moderate-severe hyperkalemia
Hyperkalemia • Hyperkalemia (K+ 8.7 mEq/L) secondary to acute renal failure • Symmetric peaked ("tented") T waves associated with potassium levels in excess of 6 mEq/L • Broad and flattened P waves that precede frank sino-ventricular conduction seen with severe hyperkalemia (i.e. conduction from the sinus node to the ventricles through specialized inter-nodal tissue without atrial depolarization) • This conduction pattern may simulate a junctional rhythm • The narrow QRS complex in this tracing is somewhat atypical for severe hyperkalemia
Hyperkalemia • Hyperkalemia (7.6 mEq/L) secondary to renal failure • Findings consistent with severe hyperkalemia • QRS widening • Peaked T waves • PR interval prolongation • P wave flattening • LBBB? Not likely with extreme QRS prolongation and other findings • If untreated, will progress to a sinusoidal pattern and eventually asystole
Hyperkalemia • K+ 10.5 mEq/L • Wide QRS with no evident P waves • ST elevations were likely due to hyperkalemia (cardiac enzymes were normal)
Hyperkalemia • Extremely wide complex rhythm (QRS 0.28 sec) at 70 bpm • Pattern approaching “sine-wave” morphology indicative of severe hyperkalemia • Atrial activity is not apparent • Serum potassium level ½ hr before 6.8 mEq/L (and likely higher at the time of this ECG) • End-stage renal disease BUN 78 mg/dL and serum creatinine 5.2 mg/dL • Emergency therapy of hyperkalemia is required based on this ECG finding
Hyperkalemia - Summary • ECG changes roughly correlate with K+ level • Early changes include peaked T waves, shortened QT interval, and ST changes • Followed by widening of the QRS, increases in PR interval, decreased P wave amplitude • Without treatment, P wave eventually disappears and QRS widens to resemble a sine wave, ventricular fibrillation or asystole follows • Life-threatening arrhythmias can occur without warning at almost any level of hyperkalemia
Hypokalemia • Sinus bradycardia with diffuse T wave flattening or inversions and markedly prominent U waves • Best seen in leads V2 and V3 • Most common causes • Hypokalemia (K+ here was 2.4 mEq/L) • Drugs such as quinidine, phenothiazines, tricyclics • Patients with hereditary long QT syndromes may show a similar finding • Pattern is of great importance because it identifies patients at high risk of torsade de pointes
Hypokalemia • Very (!) prominent U waves with Q-T(U) prolongation • Severe hypokalemia (1.5 mEq/L) due to diarrhea • Calcium was normal (remember pure hypocalemia prolongs ST segment primarily but doesn't give large U waves) • Obviously, this acquired-type long-QT(U) syndrome puts subject at risk for torsade de pointes
Hypokalemia - Summary • EKG findings may be observed as follows • Flattening of the T wave, which is the earliest change • A "U wave" then develops, associated with ST-T wave flattening and sometimes slight ST depression • ST depression is more noticeable and the U wave increases in amplitude until ultimately the U wave overtakes the T wave. • At this point distinguishing between the T wave and U wave may be almost impossible ("Q-U" prolongation).
Hypercalcemia • Hypercalcemia • Very short ST segment with a consequently short QT interval • Prominent U waves (esp. in V3) • QTc inversely proportional to the calcium level up to 16 mg/dl • At higher levels, the T wave begins to prolong, essentially making the QT interval normalize, though the ST segment remains short • In addition, prominent U waves are often seen • Chief causes of short QT are hypercalcemia and digoxin therapy (associated with characteristic "scooping" of the ST-T complex) • May cause AV block, sinus arrest, SA block, V Tach. Cardiac arrest reported, usually with rapid IV injections of calcium • This patient's serum calcium was 16 mg/dl secondary to hyperparathyroidism
Hypercalcemia • Classic (!) ECG changes • Ca++ 13.9 mg/dl • Very abbreviated ST segment such that the T wave looks like it takes off directly from QRS in some leads • High take-off of ST segment in V2/V3 is also sometimes seen in this context • Hypocalcemia is just the opposite: • Prolonged QT due to long ST segment (corresponding to changes in action potential plateau phase duration)
Hypercalcemia • Sinus rhythm at 70 bpm (with short sinus pause at the beginning) • Shortened Q-T interval (about 280 msec) and markedly abbreviated ST segment consistent with hypercalcemia • Subtle “doming” of the ST-T complex in leads V1-V3 with slight J point/ST elevations in the right chest leads is also sometimes seen in this setting • Serum calcium very elevated at 14.8 mg/dL (normal range 8.4-10.2) • Diagnosis was primary hyperparathyroidism
Hypocalcemia • Ca++ 8.2 mg/dl with minimally low albumin in patient post thyroidectomy • QT prolongation because ST segment is stretched out • Secondary to prolongation of the plateau phase of action potential • Ventricular repolarization can also be long because of 1) wide QRS; 2) flat, wide T waves (e.g. quinidine, sotalol, hypokalemia, etc); and/or 3) prominent U waves melding with T wave • The latter two syndromes, representing dispersion of ventricular refractoriness, are most likely to be associated with torsade de pointes.
Hypocalcemia • Acute pancreatitis • Sinus tachycardia • Long QT/QTc (.34 sec/.46) • Low limb lead and lateral QRS voltages • Non-diagnostic slow R wave progression V1-V3 • Non-specific ST-T changes • Long QT (ST segment component is stretched out) is due to hypocalcemia (Ca++ 7.2 mg/dL with serum albumin of 2.7 g/dL) • Sinus tachycardia is due to neuroautonomic activation in this context and the low voltage is consistent with ascites/anasarca
Hyperthyroidism • Atrial fibrillation with RVR • Left ventricular hypertrophy • Patient was markedly hyperthyroid • 5-15% of patients (esp. elderly) with hyperthyroidism will develop atrial fibrillation • Conversely, 5% of patients with recent onset atrial fibrillation (or fluuter) will have hypothyroidism
Digoxin Toxicity • Atrial fibrillation with a slow (average rate around 38 bpm) ventricular response • ST-T complexes (“scooping” of the ventricular repolarization waveform) are consistent digoxin effect (not necessarily toxicity) • In concert with the rhythm findings, digitalis excess is strongly suggested • The patient’s digoxin level was in fact in the toxic range at 2.2 nanograms/ml • The ECG also shows left ventricular hypertrophy (LVH) due underlying aortic stenosis • The ST-T abnormalities may in part be due to the LVH or to ischemia • Digitalis toxicity in the presence of atrial fibrillation may cause excessive slowing and/or regularization (due to AV junctional mechanisms) • Digitalis glycoside toxicity causes a variety of bradyarrhythmias by augmenting cardiac vagal tone at the AV node (as in the case here) or SA node • Cardiac glycoside poisoning can also occur from ingestion of various plants (e.g., foxglove) and animal toxins (e.g., venomous bites from the cane toad (Bufo marinus) • Severe digitalis intoxication can also lead to marked hyperkalemia via Na+/K+ pump inhibition • Serum potassium in this case was normal
TCA Overdose • Key findings of TCA overdose • Obtunded • Sinus tachycardia • Wide QRS / intraventricular conduction delay • Long QT • IVCD in these cases is often associated with a terminal S wave (rS) in lead I, and a terminal R wave (qR) in aVR • P waves are difficult to see (V1, for example) and in some leads (II, aVF) appear to merge with the end of the T wave