Download

1 / 42
420 likes | 593 Views
Building a Quality Framework for TCs – the development of the ATCA Standard EFTC Conference, Prague 2013 Dr Lynne Magor-Blatch Associate Professor Executive Officer ATCA. The Australasian Therapeutic Communities Association (ATCA).

E N D
Building a Quality Framework for TCs – the development of the ATCA Standard EFTC Conference, Prague 2013 DrLynne Magor-Blatch Associate Professor Executive Officer ATCA
The Australasian Therapeutic Communities Association (ATCA) • The ATCA is the peak body representing therapeutic communities in Australia and New Zealand. • Therapeutic Communities were first established in Australia in 1972 (WHOS), although many Australasian programs which later developed into TCs as understanding of the model grew, commenced in residential settings in the 1930s and 1940s, often supporting people with alcohol dependencies (e.g. The Salvation Army). • The movement formalised in Australia in 1985 during the Premier’s Conference, held in Melbourne, Victoria, and the ATCA established in 1986.
ATCA Membership • The current membership of the ATCA stands at: • 8 Group Members operating 27 Therapeutic Communities across different sites, inc community and prison-based TCs • 18 Organisational Members operating 18 TCs and community-based services • 8 Provisional Members, working through the ATCA Standard and peer review process to become full Organisational or Group members • 7 Affiliate Members, inc Individual and Organisational. Two of these working to establish TCs • Total Membership = 41 operating 62 TCs in Australia and New Zealand, 12 of which are in prison settings (9 in NZ, 3 in Australia)
ATCA Membership • In past 12 months, ATCA members: • Admitted more than 9,200 residents into TCs • 1,750 in custodial TC settings • Programs working with families admitted more than 250 children along with their parents and provided child care and child psychology services • 23,500 people seen in outpatient, education and other support services • Total of 34,700 residents and clients – an incredible record of achievement by our members Page 5
ATCA membership • TCs vary in size and are modified to meet the needs of resident populations • Largest programs are the Odyssey Houses in Sydney and Melbourne, accommodating up to 100 people • Smallest programs have less than 20 residents • Day TC programs, outpatient and education services, including health services and youth mental health programs (headspace)
ATCA membership • Prison-based TCs – 9 in NZ and 3 in Australia – all but one managed as partnership between in NGO TC and Govt Corrections • 2 Members operating 3 Youth TC programs in NSW, ACT and Vic Solaris TC • 8 Members providing Family Programs – 1 in each State/Territory of Australia except Tas & 1 NZ • 5 Aboriginal & Torres Strait Islander programs in NT, Qld and NSW, all others working with Indigenous populations
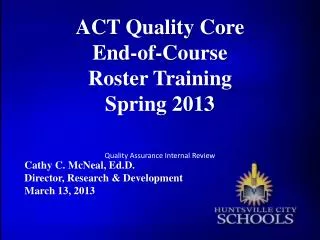
Adult Men Adult Women Adult Men Adult Women Community-based Juvenile Offenders – Community and Custodial settings Prison-based NA-based Criminal Justice-based TCs AA-based 12-Step based TCs Evolution of the TC in the last 50years in the Australasian context Adolescents Modified TCs Faith based TCs Co-occurring Disorders Day & non-residential TCs Christian-based Transitional (short-term) TCs Anglican Salvation Army Couples inc Same-sex Gender-specific Families Catholic Church Men-only Men &/or Women and Children Couples with Children Women-only Other Christian-based Uniting Care
History of CHASP and QIC standards • The Community and Health Accreditation and Standards Program (CHASP) began in 1987 using a continuous quality approach to assist organisations with primary health care service development. • In 1997 CHASP became the Quality Improvement Council Inc (QIC) with CHASP as one of its programs. Service standards developed or revised since 1997 are no longer called CHASP, but have been renamed QIC Health and Community Services Standards. They are international standards with the program operating throughout Australia and New Zealand. • Information provided by Institute for Healthy Communities Australia Inc., Qld Page 11
ATCA Peer Review • Since its inception in 1986, a major concern for ATCA has been the implementation of program evaluation processes as required by both funding agencies and management committees. • In addition to individual program evaluations, ATCA recognised the need to assist member agencies to continually improve service delivery, therefore the review mechanism selected was a Quality Assurance task conducted as a Peer Review. • A working party was formed to develop the ATCA Peer Review Manual, borrowing heavily on review processes developed by several other groups ie “Drug and Alcohol Review System” D.A.S.C.(SA), the “Standards for Residential Treatment Services” - WFTC, and the Standards for Residential Services” developed by a NSW expert committee.
History of the ATCA Standard • 1991 – First funding for Peer Reviews in the sector • 1992 – First reviews occur • 1996 – Review system was updated • Up to 2001, 2 peer reviews annually • 2002 - the Australian Government funded the ATCA for the Towards Better Practice in Therapeutic Communities project Recommendation 2: Consideration needs to be given to which components of the MEEQ are most relevant to routine monitoring and quality assurance aspects. Extraction of these components into much shorter instruments is desirable for efficient application.
The statements of the essential elements were ordered in three broad categories, with subcategories of related elements: 1. TC Ethos (reflecting the nature of the TC environment which provides a background context to intervention): (i) Nature of substance abuse and recovery (ii) Broad concept of TC approach (iii) Dimensions of socialisation (iv) Psychological/behavioural dimensions 2. Aspects of program delivery (reflecting the components of intervention experienced by residents of TCs): (i)Ensuring a safe environment (ii) Encouraging community spirit and a sense of belonging (iii) Program structure (iv) Encouraging behavioural change (v) Treatment planning (vi) Treatment components (vii) Staffing dimensions
Quality assurance (more routine aspects that are important to ensuring that TCs operate in accordance with current health care standards). The Australasian TC Essential Elements (ATCEE) were previously known as the Modified Essential Elements Questionnaire (MEEQ) and were drawn from the Survey of Essential Elements Questionnaire (SEEQ) which was developed in the USA by Melnick & De Leon (1999). These were modified to better define the therapeutic community approach in Australia and New Zealand. As for the SEEQ, the MEEQ was designed to support research and evaluation activities. The consultation that informed the development of the TC Standards provided evidence that the sector did not have a sense of “ownership” of the MEEQ, and the term “modified” was confused with the category of modified TCs. Therefore, the MEEQ is now referred to as the Australasian TC Essential Elements (ATCEEs). Page 15
History of the ATCA Standard The ATCEEs are presented under three broad headings: 1. TC Ethos (21 statements) 2. Aspects of program delivery (50 statements) 3. Quality assurance (8 statements) In 2005, the ATCA undertook the Future Directions project, which articulated recommendations from the membership regarding future directions for the Association, with a key recommendation: To provide leadership, advocacy and representation of the therapeutic community model to the broader community.
Influences on the development of the ATCA Standard • Community of Communities (C of C) is a standards-based quality improvementprogram bringing together Therapeutic Communities (TCs) in the UK and internationally, engaging them in service evaluation and quality improvement using methods and values that reflect their philosophy . • The first edition of the TC Service Standards for Addiction TCs was a product of the collaboration led by the Royal College of Psychiatrists and the Association of Therapeutic Communities (ATC) through their Community of Communities Network and including senior and practitioner representatives from the European Federation of Therapeutic Communities (EFTC) and the Australasian Therapeutic Communities Association (ATCA). Page 17
2008-2009 ATCA Standards Project • In Australasia (Australia and New Zealand) the ATCA took this work further through the support and financial commitment of the Australian Government to develop the ATCA Standard for Therapeutic Communities and Residential Services. • With new work commencing in Australia in the development of a National Quality Framework for Alcohol and other Drug Services, the ATCA's work now plays a vital role. • The first edition of the ATCA Standards and Support Package, comprised a hard copy manual and access to web based materials comprising: • 8 Standards provided as Modules • 43 Indicators • Training materials to enable TCs to undertake Self-Review and prepare for Peer Review. Page 18
2008-2009 ATCA Standards Project Objective in developing a set of service standards was to ensure the integrity of the “Therapeutic Community” principle would be maintained and continue to stand as a model of best practice in the treatment of substance misuse and co-occurring disorders. The set of standards aimed to: • Identify and describe good TC practice which can be incorporated into a national quality framework • Enable Therapeutic Communities to engage in service evaluation and quality improvement, using methods and values that reflect the TC philosophy • Develop a common language which will facilitate effective relationships with all jurisdictions (national, state and territory) • Provide a strong network of supportive relationships • Promote best practice through shared learning and developing external links. Page 19
2008-2009 ATCA Standards Project • Consultation undertaken in two phases: • The first was with approximately 60% of the Australasian TC sector, including CEOs and managers, staff, resident members and board members. • This resulted in a draft set of service standards and an outline for the Support Package. • The second phase consultation involved, wherever possible, the rest of the Australasian TC sector, and was used to refine the TC Standards and Support Package. • The significant participation by ATCA members (CEOs, managers, staff, consumers and board members) in the process is a demonstration of the solidarity and goodwill within the TC sector. The ATCA Standard, as such, has been developed by the sector for the sector. Page 20
First Conceptualisation of the ATCA Standard • The first edition of the ATCA Standard focused on eight significant health care areas and corresponding modules: • Appropriate and timely service provision; • Leadership and management principles; • Consumer participation; • Strategic human resource management; • Information management and appropriate use/evaluation of data; • Occupational health and safety; • Health and safety risk management; and • Continuous improvement. • Each Indicator was categorised as one of the following: • Essential: Indicators that demonstrate the service is a TC; • Expected: Indicators that are expected to be demonstrated by the TC sector; • Desirable: Indicators that demonstrate further best practice Page 22
Example: Standard 1 - Appropriate and Timely Service Provision – 8 Indicators • The TC program applies the Community as Method approach (Essential) • The TC program has distinct stages covering assessment/orientation, treatment, transition and re-entry (Essential) • The TC approach is multidimensional, involving therapy, education, values and skills development, and flexibly meets the needs of individuals accessing the service (Essential) • Community resident members are informed of the TC’s underlying values and principal rules at assessment and/or prior to admission, and are supported throughout the program to understand the underlying values of the TC’s service and the rationale of consequences for any breaches of the rules (Desirable)
Example: Standard 1 - Appropriate and Timely Service Provision – 8 Indicators • Staff induction and in-house training incorporates the Australasian TC Essential Elements (Expected) • During recruitment potential staff are informed of the TC’s underlying values to ensure best fit between the individual staff and the TC (Expected) • Assessment takes into consideration the resident member’s health and safety risk factors, staff skills, and the capacity of the service to inform appropriate treatment matching either at the TC and/or via referral to another service (Expected) • The Australasian TC Essential Elements are used to review the practices and the continuous quality improvement of the TC (Desirable)
First conceptualisation of the ATCA Standard • Standard 2 - Leadership and management principles (5 Indicators - 1Essential, 1 Expected, 3 Desirable) • Standard 3 - Consumer participation (6 Indicators – 1 Essential, 5 Expected) • Standard 4 - Strategic human resource management (6 Indicators – 1 Essential, 2 Expected, 3 Desirable) • Standard 5 - Information management and appropriate use/evaluation of data (6 Indicators – 1 Essential, 1 Expected, 4 Desirable) • Standard 6 - Occupational health and safety (4 Indicators – 4 Expected) • Standard 7 - Health and safety risk management (5 Indicators – 5 Expected) • Standard 8 - Continuous improvement (3 Indicators – 1 Essential, 1 Expected, 1 Desirable) Page 25
Process of Reviews • The introduction of the ATCA Standard has supported TCs to undertake a self-review, using the worksheets provided within the manual and on the website • Support offered by ATCA through Project Officer Bec Davey, who has worked with the ATCA for the past 2 years, following the initial 12 month project which was managed by Jill Rundle through funding from the Australian Government • Following self-review, a Peer Review undertaken by trained TC review team • To date, 15 reviews undertaken with 3 Provisional Members moving to full Organisational status, rural and metropolitan • 3 reviews in prison TCs (2 in NZ and 1 in Australia) and 1 Aboriginal service Page 26
The further development of the ATCA Standard • In Australia and New Zealand, it is a requirement of funding bodies that all organisations providing health services be appropriately accredited to ensure the quality delivery of services • Currently accreditation bodies do not include a standard suited to a TC or residential AOD setting – but are more suited to hospital-based or other healthcare settings • In 2011, further funding was received from the Australian Government to continue the development of the ATCA Standard, and to certify it through the Joint Accreditation Systems Agency of Australia and New Zealand (JAS-ANZ) INTERPRETIVE GUIDE TO THE AUSTRALASIAN THERAPEUTIC COMMUNITIES ASSOCIATION STANDARD FOR THERAPEUTIC COMMUNITIES AND RESIDENTIAL REHABILITATION SERVICES First Edition July 2013
The ATCA Standard • The newly developed Interpretive Guide provides two levels of accreditation. • The first level of the Standard allows an organisation to gain accreditation against a set of indicators that are directly applicable to a residential rehabilitation service for alcohol and other drug use. • For services considering a transition to the therapeutic community model, working with this Standard will assist in providing guidelines to the expectations of a service that is a TC. • To achieve accreditation as a residential rehabilitation service it is proposed agencies will need to meet 80% of criteria numbers 1–6 labelled as ‘essential’. • This represents the minimum level of activity required to demonstrate competency in agency practice in the residential rehabilitation setting.
The ATCA Standard • The second level of the Standard allows an organisation to seek accreditation as a therapeutic community. • To achieve accreditation as a Therapeutic Community, 80% of all criteria labelled as ‘essential’ must be achieved (criteria 1–13). • Performance Expectation 7.1 “Community as Method” must be within the 80% of achieved criteria. • The essential criteria relate to what policies and procedures should be in place, and how agencies identify with the therapeutic community model. • The service delivery needs of the target community and what management, staff and consumers of the agencies should know about the therapeutic community model and delivery are also encapsulated within the criterion.
Essential and Good Practice Elements • For agencies that have participated in other quality accreditation programs, a further set of criterion, called ‘good practice criteria’ has been developed. These criterion are intended to reflect what are sometimes referred to as ‘systems elements’ and are primarily related to monitoring and evaluation of agency practices. • Your agency will be awarded ‘good practice’ accreditation if, in addition to meeting all of the essential criteria, all of the ‘good practice’ criteria are met.
Performance Expectations: all services • Performance Expectation 1: The Residential Community • Performance Expectation 2: Resident Member • Performance Expectation 3: Strategic Human Resource Management • Performance Expectation 4: Information Management and Appropriate Use/Evaluation of Data • Performance Expectation 5: Workplace Health and Safety • Performance Expectation 6: Health and Safety Risk Management
Performance Expectations: TC services • Performance Expectation 7: Community as Method • Performance Expectation 8: Therapeutic Community Leadership and Management Principles • Performance Expectation 9: Therapeutic Community Resident Member Participation • Performance Expectation 10: Therapeutic Community Strategic Human Resource Management • Performance Expectation 11: Use of Data from the Therapeutic Community • Performance Expectation 12: Rules in the Therapeutic Community • Performance Expectation 13: ContinuousImprovement
Performance Expectation 7: Community as Method The agency operates in a manner that reflects the Community as Method approach and implements that in all aspects of the service. Performance Expectation 7.1: The TC programme applies the Community as Method approach. Essential Criteria a. The Therapeutic Community programme applies the Community as Method approach b. The Therapeutic Community has distinct stages which cover assessment, orientation, treatment, transition and re-entry c. The Therapeutic Community approach is multidimensional. It involves therapy, education, teaching values, and skills development
Good Practice Criteria d. The agency has established culturally appropriate and community suitable encounter measures. e. The agency demonstrates a community that is self-reliant and self-aware and deals with community issues utilising all of community measures. f. The resident group is charged with assessing readiness for stage change and providing feedback on progress through the stages. About this Standard: A profound distinction between the TC and other treatments and communities is the use of community as a method for changing the whole person (De Leon 2000: p 92). The fundamental assumption underlying community as method is that individuals obtain maximum therapeutic and educational impact when they meet community expectations for participation in and use of the community context to change themselves (De Leon 2000: p 98).
The Future of the ATCA Standard • The ATCA Standard is in the final stages of certification, which will then make it available through the market to independent Certifying Assessment Bodies (CABs) to be used for accreditation. • ATCA retains the licence and will require that all accreditation reviews are undertaken with a TC ‘expert’ as part of the team. That expert will focus on the elements of the full standard that relate directly to the TC model. • The ATCA Standard will be able to be linked directly to the ISO 9000 business management systems Standard meaning an organisation with any number of other services can undertake the ATCA Standard review in conjunction with all other accreditation reviews. • This reduces the workload on the organisation and streamlines all accreditation activities and removes the onus on the ATCA to be the expert in all manner of business systems – it only has to focus on the TC model in which it is an expert • . Page 29
The Future of the ATCA Standard • Therefore, the ATCA Standard will include only those standards that are applicable to the TC process • In conjunction with the full Standard certified by JAS-ANZ, the ATCA will maintain a modified version to apply through a peer review process • These elements will be the same as those which the TC expert on an ISO accreditation visit reviews, but allows for organisations who do not wish to undertake the full ISO accreditation to maintain their requirements against membership to the ATCA • The peer review is necessary for all new members to bring them from Provisional status (granted on becoming a member of the ATCA) to Full Organisational or Group Membership status • It may also serve as a “dry run” for TCs wishing to ensure they have all ATCA requirements in place and can meet accreditation prior to the external review • This will be conducted by ATCA reviewers on fee-for-service basis Page 30
Activity in the National Arena • The Australian Government currently has 2 important processes in place – Review of the AOD Service Sector & AOD Quality Framework Project. • Review – project undertaken by the Drug Policy Modelling Project (DPMP) lead by Prof Alison Ritter (NDARC; Prof Michael Farrell is Director) • Guided by and Expert Review Committee – A/Prof Lynne Magor-Blatch (ATCA) is member. • Quality Framework Project – project lead by Turning Point (Melbourne) and headed up by Prof Dan Lubman and A/Prof David Best with expert team – and includes A/Prof Lynne Magor-Blatch (ATCA). • Tasked with the development of quality framework for all Government funded AOD services. • Both projects to be completed by June 2014. Page 30
TC Training • In Australia, jurisdictions adopting a “minimum qualification” standard – Certificate IV in AOD work, provided by VET sector. • In Australia, AOD training also offered at Graduate and PG university level. • In NZ, undergraduate university training also offered. • ATCA supported by the NZ Ministry of Health to develop TC training – including both accredited or non-accredited training. • In NZ this is being led by MatuaRaki, the AOD Workforce Development organisation. • Joint survey – closed on Monday. • 501 responses (265 NZ, 236 Australia) Page 30
TC Training: Survey results • What is your professional background? Aus: AOD Worker 56.3% (134) Aus/NZ: AOD Worker 27.2% (135); Addiction Specialist 24.5% (122) 2. Specify your highest qualification: Aus(Aus & NZ) Page 30
TC Training: Survey results 3. If you were able to undertake a course or module that covered TC theory, process and experience, would you be interested? Aus: 86.6% (206) - YES Aus/NZ: 85.0% (425) - YES 4. Would you prefer toundertake a TC course through… Aus: Workshop - 56.4% (114); Training Institute – 36.1% (73); Online & In TC – 32.7% (66) Aus/NZ: Workshop – 60.2% (245); Training Institute – 37.1% (151); Online – 31.2% (127) 5. At what level would you prefer this course to be taught? Aus: TAFE as component of Cert IV/Diploma - 63.4% (128). Aus/NZ: TAFE Cert IV/Diploma - 31.4% (128); PG – 27.0% (110) Page 30
TC Training: Survey results 6. What is more important to you? Aus: Both accredited and non-accredited – 46.5% (94); Accredited – 42.6% (86) Aus/NZ: Both accredited and non-accredited – 23.1% (94); Accredited – 21.1% (86) 7. Position in TC Aus: Currently working in TC – 69.5% (162); Manager TC – 15.5% (36) Aus/NZ: Currently working in TC – 43.9% (213); Not working in TC and unlikely to– 16.7% (81) 8. If you are managing a TC, would you have the resources (payment of fees, backfill etc) to support your staff undertaking this training? Aus: No – 56.7% (17); Yes – 43.3% (13). Aus/NZ: Yes – 51.0% (26); No -49.0% (25). Page 30
TC Training: Survey results 9. What type of training did you receive for your work in a TC? Aus: In-house theory and experiential – 58.8% (120); I have been a resident prior to becoming a staff member – 27.9% (57); Theory covered in my qualifications – 22.5% (46) Aus/NZ: In-house theory and experiential – 60.3% (188); Theory covered in my qualifications – 26.3% (82) • Next step – Project groups established in Australia and New Zealand to develop training. Likely to be offered through face to face workshops and online training as TC module as part of TAFE qualification, supported by placements in Adult, Youth, Family and Prison-based TCs. • Offered through RTOs (3 ATCA members are RTOs in Australia and would therefore take the lead in providing training. Page 30
Want to know more? Email Lynne Magor-Blatch, Executive Officer atca@atca.com.au Or…. Visit the ATCA website (about to go “live” with new upgrade) – www.atca.com.au ATCA acknowledges the Australian Government Department of Health and Ageing (DoHA) for their financial support of the ATCA Secretariat and the development and implementation of the Australasian Alcohol and other Drug Therapeutic Communities Standards & Training package.