PROCEDURES
PROCEDURES. INFORMED CONSENT. DEFINITION: Process that fosters patients’ participation in the planning of their care. Required by hospital policy and Ohio law. Just signing a piece of paper leaves the “informed” piece out of informed consent.

PROCEDURES
E N D
Presentation Transcript
INFORMED CONSENT • DEFINITION: • Process that fosters patients’ participation in the planning of their care. • Required by hospital policy and Ohio law. • Just signing a piece of paper leaves the “informed” piece out of informed consent. • You do not have to get informed consent in an emergency
INFORMED CONSENT • Elements of Informed Consent • Purpose and nature or procedure/treatment • Expectations of procedure/treatment • Risks of procedure/treatment • Alternatives to procedure/treatment and the risks/benefits of the alternatives • Names of physicians involved • Answer any questions • Signature of patient or authorized individual
INFORMED CONSENT • Patients must have capacity to make decisions in order to consent to procedure/treatment. • Capacity is defined as the ability to… • Understand information they are given • Apply information to their situation • Reason/deliberate about the choices available • A patient who has capacity can refuse medical care. • If the patient does not have capacity, then the informed consent process should be obtained from POA or next of kin.
Central Venous Catheters • Indications • Administration of caustic medications • Invasive monitoring (CVP, SVO2) • Large volume resuscitation • Dialysis • Plasmapheresis • Inability to obtain PIV • Contraindications • Infection at insertion site • Coagulopathy • Thrombocytopenia • Thrombosis of target vessel
Central Venous Catheters • Complications • Arterial stick or cannulation • Hematoma • Pneumothorax • Hemothorax • Retained wire • Air embolism • Bleeding • Infection • Arrhythmias • Catheter related thrombosis • Vascular perforation • Site Selection • Minimize infection choose SC > IJ > femoral • Choose compressible site if concerned about bleeding • Avoid SC if bilateral lung pathology • Avoid placement of IJ/SC on side of unilateral lung pathology
Arterial Lines • Indications • BP monitoring • Titration of vasopressors • Frequent ABGs • Contraindications • Infection at insertion site • Failure to demonstrate collateral flow (Allen test)
Arterial lines • Complications • Retained guide-wire • Infection • Hematoma • Limb ischemia
Thoracentesis • Indications • Evaluation of new pleural effusion • Respiratory compromise • Suspected infection • Suspected malignancy • Contraindications • Infection at insertion site • Coagulopathy • Thrombocytopenia • Bullous lung disease
Thoracentesis • Complications • Pneumothorax (5-10%) • Hemothorax (1%) • Re-expansion pulmonary edema • Pleural Fluid Analysis • LDH • Protein • Cell count with diff • Gram stain • Culture • Additional studies as needed
Thoracentesis INTERPRETATION OF RESULTS • Light’s Criteria for exudative effusion = • Protein (pleura) / Protein (serum) >0.5 • LDH (pleura) / LDH (serum) >0.6 • LDH (pleura) >2/3 upper limit normal • Exudativeneutrophil predominant = infection • Exudative lymphocytic predominant = TB, cancer • Complicated parapneumonic = +gram stain, pH <7.2 or glucose <60 • ADA >70 = suggests TB • Glucose <60 = suggests infection, cancer, RA • Hemothorax = effusion Hct/serum Hct >50%
Lumbar Puncture • Indications • Suspected CNS infection • Suspected SAH • Suspected CNS malignancy • Evaluation of demyelinating /inflammatory CNS process • Therapeutic reduction of CNS pressure • Delivery of intrathecal chemotherapy • Unexplained headache • Contraindications • Infection at insertion site • Elevated ICP • Mass lesion of spinal cord or brain • Coagulopathy • Thrombocytopenia
Lumbar Puncture • Indication for Head CT prior to LP: • Age >60 years • h/o seizures or CNS disease • Immunocompromised state • Focal neuro deficit • Decreased LOC • Papilledema • Complications • Post LP Headache • Backache at site of puncture • Infection • Bleeding • Spinal hematoma • Brain herniation • Neuropathic pain of lower extremities
Lumbar Puncture • CSF Analysis • Glucose • Protein • Cell count with diff • Gram stain & culture • Additional studies as needed • Viral culture • PCR ofr HSV, EBC, CMV, enterovirus • VDRL/FTA • Cytology • Oligoclonal bands • Fungal and acid-fast stains/cultures • INTERPRETATION OF RESULTS • Normal OP = 9-18cm • Elevated with infection, hydrocephalus, pseudotumor • Normal Glucose = 50-70 • Decreased in infection • Normal Total Protein = 15-40 • Elevated in infection, MS, tumors, hemorrhage • Can be artificially elevated if RBC elevated (subtract 1mg protein/dL for every 1000 RBC count) • Normal WBC = <5 • PMN = bacterial • Lymphocytes = TB, fungal, aseptic • Can be elevated with elevated RBC (subtract 1 WBC from measured WBC for every 700 RBC’s in CSF) • Normal RBC = 0 • Elevated in traumatic tap, SAH
Paracentesis • Indications • Evaluation of new ascites • Suspected spontaneous or secondary bacterial peritonitis • Symptomatic control of shortness of breath in massive ascites • Contraindications • Infection at insertion site • Coagulpathy(controversial) • Thrombocytopenia (controversial) • Severe bowel distention • Full bladder
Paracentesis • Complications • Infection • Hematoma • Persistent leak of ascites • Bleeding • Bowel perforation • Renal failure • Hemodynamic instability including hypotension/ARF • ***For large volume taps (>4L) give 6-8g/L of 25% albumin • Fluid analysis • Cell count with diff • Gram stain & culture (direct innoculation of cx bottles at bedside) • Additional studies as needed • Glucose (<50mg/dL suggests perforated viscus) • LDH ratio of ascites:serum(1=SBP, >1 =cancer/infxn, <1 = uncomplicated cirrhosis) • Amylase ratio of ascites:serum(>3 suggests pacreatitis) • Triglycerides >200mg/dLsuggests lymphatic obstruction, cancer, TB • Cytology
Paracentesis INTERPRETATION OF RESULTS • SAAG = serum albumin – ascites albumin ≥ 1.1 = portal HTN related ≤ 1.1 = non-portal HTN related • Ascites fluid total protein (use when SAAG >1.1) > 2.5 = suggests cirrhosis < 2.5 = suggests heart failure • WBC > 500 or PMNs >250 = suggests infection
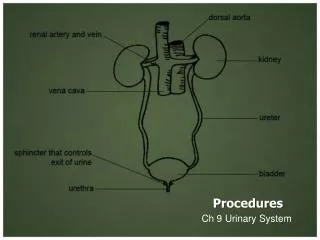
Foley Catheter • Indications • Acute urinary retention • Bladder outlet obstruction • Urine output measurement in critically ill patients • Continuous bladder irrigation • During surgery • Management of open wounds in perineal region • Intravesical pharmacologic therapy • Contraindications • Urethral injury associated with pelvic trauma • Urethral stricture • Artificial sphincter • Complications • Infection • Retained balloon fragments • Bladder fistula • Bladder perforation • Bladder stones
Picc Line • Indications • Administration of caustic medications • Inability to obtain PIV • Outpatient antibiotic administration • Contraindications • Infection at insertion site • Coagulopathy • Thrombocytopenia • Active bacteremia • Venous stenosis • Complications • Arterial stick or cannulation • Hematoma • Pneumothorax • Hemothorax • Retained wire • Air embolism • Bleeding • Infection • Arrhythmias • Catheter related thrombosis • Vascular perforation
Arthrocentesis • Indications • Diagnosis of joint effusion • Suspected septic joint • Establish diagnosis in arthritis • Drainage of blood from hemarthrosis • Pain relief with large effusion • Suspected inflammatory arthritis • Contraindications • Infection at the insertion site • Bacteremia • Coagulopathy • Thrombocytopenia
Arthrocentesis • Compliations • Bleeding • Infection • Exacerbation of arthritic pain • Synovial fluid analysis • WBC • Gram stain and culture • Glucose • Protein • Crystal exam
OTHER • For invasive procedures goal INR <1.5 and platelets >50,000 • Remove invasive lines/tubes as soon as possible to prevent infection • Be aware of blood and body fluid exposure guideline • Be aware of Universal precautions • Review videos of procedures on New England Journal of Medicine website