Download
1 / 14
140 likes | 294 Views
Role of biologic therapy in the treatment of unresectable appendiceal epithelial neoplasms. Eng C 1 , Overman M 1 , Fournier K 2 , Royal R 2 , Ohinata A 1 , Rafeeq S 2 , Phillips JK 1 ,Gajula P 1 , Wolff RA 1 , Mansfield P 2

E N D
Role of biologic therapy in the treatment of unresectableappendiceal epithelial neoplasms Eng C1, Overman M1, Fournier K2, Royal R2, Ohinata A1, Rafeeq S2, Phillips JK1,Gajula P1, Wolff RA1, Mansfield P2 The Department of Gastrointestinal Medical Oncology1, Surgical Oncology2, The University of Texas M. D. Anderson Cancer Center, Houston, Texas.
Acknowledgements • Philanthropic support was provided by the Ric Summers Appendiceal Cancer Research Fund.
Background • Appendiceal epithelial neoplasms (AEN) are a rare tumor type comprising a spectrum from indolent, well-differentiated tumors to the highly aggressive signet-ring histology1-3. • Typical patients exhibit extensive accumulation of mucinousascites and tumors within the peritoneal cavity, arising from the appendix. Since patients often present with advanced disease, treatment and management of this malignancy is difficult. • The mainstay of treatment consists of surgical debulking, or cytoreductive surgery (CRS). Surgery is combined with hyperthermicintraperitoneal chemotherapy (HIPEC) to help eradicate microscopic disease. But the procedure carries significant risk4-5, and lowers the rate of surgical candidacy of this population even further.
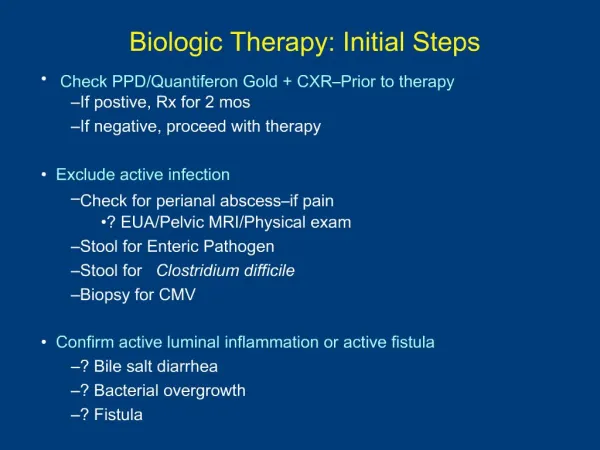
Thus, for those patients (pts) who recur, or are otherwise sub-optimal candidates for CRS, systemic maintenance therapy is considered and has been associated with a reasonable PFS and OS6, but to date there is a lack of consensus regarding an optimal chemotherapy regimen. • Given the recent advances in biologic therapy, and the concurrent costs, it is important to evaluate whether the addition of these agents to chemotherapy is of therapeutic benefit to this population.
Aim • To determine the benefit to overall survival, progression-free survival, and clinical or radiographic response following the use of biologic therapy in combination with chemotherapy in biologic-naïve, surgically unresectableappendiceal epithelial neoplasm patients.
Methods • Study Design and Population • Retrospective consecutive cohort study of biologic-naïve patients with surgically unresectable AEN, treated with systemic chemotherapy plus biologic therapy, from 2000-2010. Control cases not receiving biologic therapy were consecutively selected from the same timeframe. • Eligible patients were required to obtain all radiographic imaging at MDACC. • An appropriate waiver of informed consent was obtained. • Electronic medical records were reviewed for patient demographics, tumor characteristics, and clinical outcomes including: • Prior CRS, with or without HIPEC, histology, systemic treatment received, tumor markers (CEA, CA-125, and CA 19-9), response (R), progression-free survival (PFS), and overall survival (OS). • Best response to treatment was determined from radiographic imaging, tumor markers, and physician records. • Statistical Analysis • OS and PFS were determined using the Kaplan-Meier method. The log-rank test and Cox proportional hazard model were used for statistical comparisons.
Chemotherapy Regimens(Table 2) Biologic Agents Used in First Line(Table 3)
Results • 130 pts were evaluable for OS and PFS. Median follow up: 78 months. • Survival outcomes (Figures 1 & 2): • The addition of biologic therapy improved median PFS (8M vs. 4M, p-value = 0.08) and was statistically significant for OS (62M vs. 42M, p-value = 0.03). • Multivariate analysis indicated improved PFS (HR: 0.72; 95% CI: 0.50-1.01; p-value: 0.06) and significantly improved OS (HR: 0.55; 95% CI: 0.34-0.88; p value = 0.01) in favor of biologic therapy. • Median lines of subsequent therapy = 1 • 28 of 59 (47%) continued bevacizumab beyond progression of disease.
Treatment Response Bio vs. No Bio (Table 4) • Determination of response: • 117 pts (90%) were evaluable for response. • Best response to the regimens were recorded. • 33 (28%) pts had progressive disease. • 20 (17%) pts had a partial response. • 64 (55%) pts had stable disease. • There was a significant difference in response between those patients who received biologics compared to those who did not (p=0.02) (Table 4).
Conclusions • The use of biologic therapy, primarily anti-VEGF therapy in our analysis, in combination with chemotherapy versus systemic chemotherapy alone appears to have a role in surgically unresectableappendiceal epithelial neoplasm (AEN) patients, with a trend for improvement in PFS and clear benefit in OS. • Our analysis was underpowered to determine the role of anti-EGFR therapy as a single agent or in combination with chemotherapy but indicates further analysis should be pursued in this patient population. • Given the cost of biologic therapy, cost-benefit analyses should be pursued. Tissue/blood correlatives and quality of life analysis are currently underway. • We understand the limitations of a retrospective study with a small, select sample size. Nevertheless, we consider the results worthy of discussion for such a rare patient population.
References • Baratti D, et al: Pseudomyxomaperitonei: clinical pathological and biological prognostic factors in patients treated with cytoreductive surgery and hyperthermicintraperitoneal chemotherapy (HIPEC). Ann SurgOncol. 2008;15(2):526–534. • Yan H, et al: Histopathologic analysis in 46 patients with pseudomyxomaperitonei syndrome: failure versus success with a second-look operation. Mod Pathol. 2001;14(3):164–171. • Sugarbaker PH: Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative approach to pseudomyxomaperitonei syndrome. Tumori. 2001;87(4):53–55. • Kusamura S, et al: Cytoreductive surgery followed by intraperitonealhyperthermic perfusion: analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer. 2006;106:1144–1153. • Deraco M et al: Morbidity and quality of life following cytoreduction and HIPEC [review]. Cancer Treat Res. 2007;134:403–418. • Shapiro JF, et al: Modern systemic chemotherapy in surgically unresectableneoplasmsofappendiceal origin: a single-institution experience. Cancer. 2010 Jan 15;116(2):316-22.