Download
1 / 26
340 likes | 1.05k Views
Benign Epithelial Mesenchymal Malignant Epithelial Mesenchymal Lymphoma Carcinoid. NEOPLASMS OF THE STOMACH. Tumors of the Stomach. Tumors arising from the mucosa predominate over mesenchymal tumors. These are classified into polyps and carcinoma.

E N D
Benign Epithelial Mesenchymal Malignant Epithelial Mesenchymal Lymphoma Carcinoid NEOPLASMS OF THE STOMACH
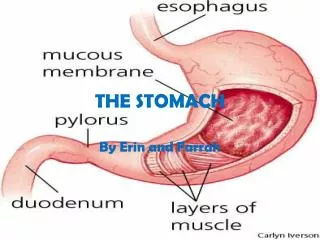
Tumors of the Stomach • Tumors arising from the mucosa predominate over mesenchymal tumors. • These are classified into polyps and carcinoma. • The term “polyp” is applied to any nodule or mass that projects above the level of surrounding mucosa • The use of the term “polyp” in GI tract is generally restricted to mass lesions arising in the mucosa.
NEOPLASMS OF THE STOMACH • Benign • Epithelial • hyperplastic polyps • Fundic gland polyps • Adenomatous polyps. • Mesenchymal • Malignant • Epithelial • Mesenchymal • Lymphoma • Carcinoid
Benign Neoplasms of Stomach • Mucosal polyps • Epithelial polyps are rare. (0.4%) • Types: • 1] hyperplastic polyps; (80% to 85% • 2] Fundic gland polyps (∼10%) • 3] Adenomatous polyps (∼5%) • Appear as sessile or small pedunculated lesions, often multiple that can be removed endoscopically. • All three types arise in patient with chronic gastritis. • Large polyps are very rare. - The risk of carcinoma is moderate in adenomatous polyp,slight in hyperplastic polyp, and nil in fundic gland polyps.
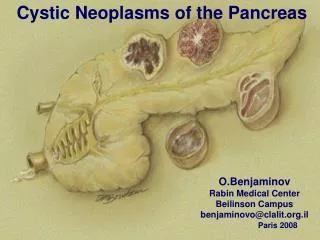
Adenomatous polyp of the stomach. Note the large size of the polyp and its lobulated configuration.A small ulceration ( arrow) can be identified on its surface.
Malignant neoplasm of stomach • Carcinoma – 90-95% • Lymphoma – 4% • Carcinoids – 3% • Malignant spindle cell – 2%
Gastric carcinoma is the second leading cause of cancer-related deaths in the world, with a widely varying geographic incidence.
Malignant neoplasm of stomach • Gastric adenocarcinoma Epidemiology • The incidence of gastric carcinoma is five to ten times higher in Japan than in the United States. It is also high in China and Chile.
There are two patterns Intestinal typeand Diffuse type . Intestinal type occur on top of ch. Gastritis and intestinal metaplasia and common in high risk population after age 50 with 2:1 male predominance Diffuse type arise de novo in younger age group with with female predominance In the United States, the incidence of Intestinal typehad declined since 1950
Gastric adenocarcinoma Risk factors for Gastric Carcinoma • Intestinal type adenocarcinoma • Diet • Nitrites • Smoked foods • Excessive salt • Decreased intake of fresh vegetables and fruits • Ch. Gastritis and intestinal metaplasia • Infection by H. pylori • Pernicious anemia • Altered anatomy • Diffuse Carcinoma Undefined, E- cadherine(50%), FGFR2 (33%)
Amplification of HER-2/NEU and increased expression of β-catenin are present in 20% to 30% of cases and are absent in diffuse carcinoma
Malignant neoplasm of stomach Gastric Carcinoma • Precancerous lesions ( intestinal type) 1. Chronic atrophic gastritis associated with pernicious anemia. 2. Chronic atrophic gastritis associated with helicobacter pylori infection. 3. Those with adenomatous and hyperplastic polyps. 4. Following subtotal gastrectomy.
Malignant neoplasm of stomach Gastric carcinoma Site: - pylorus and antrum – 50-60% - cardia – 25% - body and fundus 15 -25% lesser curvature 40% Greater curvature 12% a favored location is the lesser curvature of the antropyloric region
Malignant neoplasm of stomach Gastric carcinoma • Divided into: 1. Early gastric cancer (lesion limited to mucosa and submucosa) – appears as a small, flat mucosal thickening that may have a minimal polypoid and ulcerative component. 2. Late gastric cancer – defined as a gastric carcinoma that has invaded the muscle wall. It may present in various ways: - As a fungating mass that protrudes into the lumen. - As a diffusely infiltrating lesion that causes thickening and contraction of the stomach wall with relatively little mucosal involvement (linitis plastica, or leather-bottle stomach). - As a malignant ulcer (excavated) with raised, everted edges.
Malignant neoplasm of stomach Any gastric ulcer that does not heal as expected should be biopsied to rule out carcinoma.
Gastric carcinoma Intestinal type
The diffuse variant of gastric carcinoma • Arise de novo from native gastric-type mucous cells that generally do not form glands but rather permeate the mucosa and wall as scattered individual “signet-ring” cells or small clusters in an infiltrative growth pattern. • There is no association with chronic gastritis • Poorly differentiated • It occurs at early ages with female predominance. • Risk factors undefined • Rare inherited mutation of E-cadherin leading to autosomal dominant inheritance. • Mutations in FGFR2, a member of the fibroblast growth factor receptor family, and increased expression of metalloproteinases are present in about one-third of cases, but are absent in intestinal-type carcinomas.
Gastric carcinoma Diffuse variant Intestinal type
Malignant neoplasm of stomach Spread of Gastric carcinoma • Direct: • Invades through the muscle wall into the omental fat. • Spread of tumor cells in the peritoneal fluid. • Spread to the ovary (Krukenberg’s tumor) and rectovesical pouch. • Lymphatic metastasis • to lymph nodes around the stomach • Left supraclavicular node (Virchow’s node) • Lymph node metastases are present in about 50% of cases at the time of diagnosis • Blood stream spread to the liver and lung
Malignant neoplasm of stomach Clinical Features of Gastric carcinoma • Early gastric cancer: • asymptomatic • Late gastric cancer: • Resembling chronic peptic ulcer • Anorexia, anemias, weight loss, hematemesis and melena. • Tumors near the pylorus may cause gastric outlet obstruction.
Malignant neoplasm of stomach Prognosis of Gastric carcinoma • The prognosis depends on the depth of invasion of the neoplasm. Early cancer - 85% - 5 years survival Muscle wall invasion – 30% - 5 years survival Full thickness invasion and lymph node – 5% - 5 year survival • Histologic features and differentiation are of little prognostic importance.
Malignant neoplasm of stomach • Malignant lymphoma • Two common types occur: a. Low-grade malignant lymphoma arising in mucosa- associated lymphoid tissue (MALT lymphoma). b. High-grade aggressive B cell lymphomas, most commonly B immunoblastic lymphoma. • Present as polypoid masses, ulcers, thickened fold. • MALT lymphoma restricted to can be cured by surgical resection ( more likely to be associated with H. pylori) • High grade lymphomas respond to chemotherapy, and have a 5 year survival rate of about 60%.
Malignant neoplasm of stomach 3.Malignant gastric stromal neoplasms • Commonest mesenchymal neoplasm (2% of gastric malignancies) • Arise from undifferentiated mesenchymal cells in the gastric wall with ulceration. • Present as large masses that originate in and involve the wall with ulceration. • Composed of spindle cells that show varying cellularity, pleomorphism and mitotic activity with smooth muscle or neural differentiation. • Treatment: Surgical resection • over 50% survive 5 years.
Malignant neoplasm of stomach • Carcinoid tumors - extremely rare. - give metastasis in 30% of cases.
Summary of Gastric Tumors • More than 90% of gastric tumors are carcinomas; • lymphomas, carcinoids and stromal tumors are relatively infrequent. • The two main types of gastric adenocarcinomas are the intestinal and diffuse types; macroscopic patterns of both types may be exophytic, flat or depressed, or excavating. • Intestinal type of adenocarcinoma is associated with chronic gastritis caused by H. pylori infection, with gastric atrophy and intestinal metaplasia; composed of malignant cells forming intestinal glands. • Diffuse type of adenocarcinoma is not associated with H. pylori infection; composed of gastric type of mucous cells (signet ring cells) that permeate the mucosa without forming glands.