Slide Note
0 likes | 86 Views
Fluoride works in three ways to reduce and prevent tooth decay: systemically by being incorporated into the enamel structure, topically by promoting remineralization and inhibiting demineralization, and through community water fluoridation. This comprehensive approach has been shown to be effective in preventing dental caries since the 1930s.

E N D
نمحرلا الله مسب ميحرلا ميظعلا يلعلا الله قدص
Fluoride in prevention and controlling dental caries Dr. Rihab Abdul Hussein Ali B.D.S , M.Sc. , PhD.
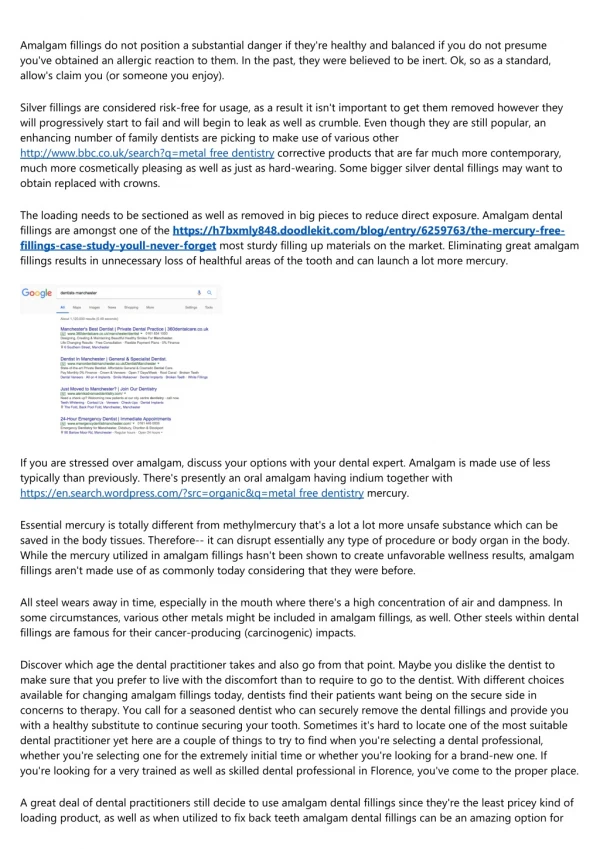
Mechanisms of action of fluoride Fluoride works in three ways to reduce and prevent tooth decay: - The First Way • Systemically by being ingested and incorporated of fluoride into the enamel structure during tooth development. The anti-caries effect of fluoride was demonstrated since 1930s. • Fluoride’s effect on tooth mineral has been studied, enamel is composed primarily (~95%) of hydroxyapatite (HA) crystals in which are substituted a number of other ions including fluoride. Well-formed HA crystals have a hexagonal configuration of phosphate and calcium ions with a central hydroxyl ion.
Unit cell of hydroxyapatite showing central hydroxyl ion surrounded by triangles of calcium and phosphate, the whole surrounded by a hexagon of calcium ions
The incorporation of magnesium and carbonate because of a poor fit in the crystal tends to destabilize the crystal, making it more susceptible to acid dissolution. In developing enamel, carbonate will substitute for phosphate ions and if the concentration is high enough for hydroxyl ions. Magnesium can substitute to a limited extent for calcium but often resides at the crystal surfaces.
Unit cell of hydroxyapatite showing the central ion (the hydroxyl ion has been replaced with a fluoride ion) and possible location of other substituent ions notably carbonate and magnesium.
Systemic fluoride when ingested, or taken into the body during consumption of foods or beverages: • It can be incorporated directly into the hydroxyapatite crystalline structure of the developing tooth with the smaller fluoride ions replacing hydroxyl ions in the crystalline structure of the tooth and producing a less‐soluble apatite crystal. • It also can provide a topical effect because saliva contains some fluoride from ingestion, is continually available at the tooth surface, and becomes concentrated in dental plaque where it inhibits acid‐producing cariogenic bacteria from demineralizing tooth enamel.
• Fluoridation is a population-based method of primary prevention designed to serve as the cornerstone for the prevention of dental caries. It was initiated in 1945 when Grand Rapids, Michigan fluoridated its public-water supply. Community water fluoridation has continued to play a dominant role in the decline in caries, even though the absolute differences in caries prevalence.
• Determination of the benefits and effectiveness of community water fluoridation should consider the state of the population’s oral health before fluoridation. The reduction in the absolute measurable benefits of water fluoridation has been attributed to the dilution and diffusion effects.
• Dilution results from the increased availability of fluoride from multiple sources, diluting the impact of any one source of fluoride, including water. Dilution is the apparent reduction in the measurable water fluoridation benefits resulting from the ubiquitous availability of fluoride from other sources in both the fluoridated and the fluoride‐deficient community.
•Diffusion referred as the extension of benefits of community water fluoridation to residents of fluoride‐ deficient communities. Diffusion results from the consumption of commercial foods and beverages that were processed in a fluoridated community and transported to fluoride‐deficient communities.
• The optimal level of fluoride is that level in drinking water causing maximum reduction of dental caries but with no clinical signs of dental fluorosis. It is a range, 0.7 to 1.2 ppm, which assumes greater water consumption in hotter climates and less water consumption in colder climates. Consequently, the higher the average temperature in a community, the lower the recommended water fluoride level.
- The Second Way • Topically by promoting remineralization and inhibiting demineralization of tooth surfaces after eruption. Regular use of fluoride products resulting in prolonged fluoride concentration in saliva, this may enhanceremineralization of enamel lesions and arrest of caries lesion.
• Fluoride encourages remineralization for two reasons. First, the solubility products of fluoride- enriched minerals are lowered. Secondly, as fluoride is incorporated into recrystallizing apatite crystals, hydroxyl groups are released, which neutralize some of the protons produced by the bacteria. The removal of protons increases the pH, and this will further drive the solubility reaction toward the precipitation of apatite.
• Mineral deposition in enamel defects may result in complete or partial replacement of the lost minerals and this called remineralization. While demineralization referred as loss of minerals resulting from partial dissolution of enamel crystals. After an acidic challenge that causes demineralization of tooth surfaces, salivary flow buffers the acids produced by the bacterial breakdown of dietary sugars in dental plaque.
• When the pH is higher than 5.5, remineralization will naturally occur because saliva is supersaturated with respect to the dental mineral. Fluoride will adsorb to the surface of the partially demineralized crystals and attract calcium ions. Because carbonate‐free or low‐carbonate apatite is less soluble, these phases will tend to form preferentially instead of the original mineral coating and will be less soluble due to the exclusion of carbonate and incorporation of fluoride, rendering the enamel more resistant to future acidic challenges.
• Fluoride ion has great affinity for demineralized regions where free calcium and phosphate ions are present. The fluoride combines the calcium and phosphate ions forming fluoride appatite (FA) is more stable than the favorite ion for fluoride (CaF2).Excess deposition of FA and CaF2 may block the pores of lesion. Formation of CaF2 is possible at fluoride concentration more than100 ppm. The dissolution of CaF2 is to its anti-caries effect. More ionic fluoride can be released during cariogenic challenge. Fluoride must be constantly present in the oral environment at low concentrations.
• Hydroxyapatite molecules are arranged in long and thin apatite crystals, which in turn are organized into the resulting enamel prisms. Despite the high mineral content, the space between the crystals is occupied by water and organic material. It is in this space filled with the enamel fluid that the de‐ and remineralization reactions take place.
• Upon a cariogenic challenge, hydroxyapatite crystals are dissolved from the subsurface while fluorapatite crystals are deposited at the surface, thus resulting in a subsurface lesion. The dissolution process of enamel is therefore a chemical event. On the other hand, dentin contains apatite, organic components, and water. Fluoride concentrations as small as 1 ppm present in an acid solution can reduce the solubility of carbonated hydroxyapatite to that equivalent to hydroxyapatite.
• During caries process, the concentration of fluoride in enamel increases. The necessary fluoride could be derived from plaque so this helps to maintain mineral levels in the surface layer of the carious lesion. Whether fluoride is optimally positioned either in or on the tooth surface, as opposed to in the plaque or plaque fluid, is debatable and could be irrelevant as long as ionic fluoride is available at the site of the developing lesion. This hypothesis is supported by a number of studies that showed the same caries reduction after topical fluoride applications with and without the prior removal of dental plaque.
- The Third Way • Topically by inhibiting glycolysis in microorganisms, thereby hindering the ability of bacteria to metabolize carbohydrates and produce acid. The most important effect of fluoride on plaque bacteria is to reduce production of acid that occur at low concentration of fluoride. The antimicrobial effect of fluoride is enhanced in combination with cations.
• Cariogenic bacteria have to thrive in an episodic low pH environment. Halfof the plaque biofilm is primarily composed of the acidogenic Mutans streptococci and Lactobacillusspecies, and the other half contains other microorganisms. • Fluoride inhibits the glycolytic enzyme, enolase, which converts 2-P-glycerate to P-enolpyruvate (PEP). This results in the inhibition of sugar transport via the PEP phosphotransferase system (PTS).
• Acidic conditions outside of the cell wall of the bacteria (when APF fluoride is applied) convert fluoride ions to hydrogen fluoride (HF), which is able to diffuse into the bacteria. Inside the cell, where the cytoplasm disassociates into fluoride ions and protons. The fluoride ions inhibit metabolic enzymes and the added protons acidify the cytoplasm, causing a reduction in both the proton gradient and enzyme activity. When fluoride inhibits the membrane-bound, proton pumping H+/ATPase, the cell’s ability to expel protons to the environment at the expense of ATP is inhibited. alkaline, HF is
• Fluoride reduces production of bacterial acids by interfering with the control of intracellular pH. The inhibition of acid production would be a consequence of cytoplasmic acidification rather than the primary effect of fluoride. Fluoride will directly affect the dissolution of tooth minerals by reducing the undersaturation.