Download
1 / 10
100 likes | 126 Views
Explore two anemia cases in a virtual lab setting. Learn to identify RBC abnormalities and analyze red cell indices for differential diagnosis. Understand symptoms, signs, and complications.

E N D
Your instructor will briefly introduce each case then ask students to work through the slides, questions, answers and virtual slides using the PowerPoint show (PPS) on their laptops. The micrographs are displayed adjacent to micrographs of a "normal" or "look-alike" abnormal smear at the same (or nearly the same, case #3) magnification. The micrographs should serve as a guide for viewing the virtual slides. The virtual slides can be accessed from links embedded in the PPS (if you are using a workstation or laptop on the Medical School Campus). A “self-test tool” for the virtual slides is available as well (self-test tool). Hematopathology Lab 1 Start Slide Show Read history, review image stacks (space bar, arrow, mouse click) Space bar, arrow, mouse click to reveal question Space bar, arrow, mouse click to reveal answers After working through case using PPS, open virtual slide (links in PPS) and review
Normal blood smear Virtual Slide Normal Smear (Web viewer)
CASE 1: A 19-year-old woman with anemia presents with a two day history of fever and joint pain. She reports experiencing similar episodes 2-3 times/year that respond to hydration and pain medication. Her history is notable for avascular necrosis of the left femoral head at age 14. Normal smear stack Patient stack Virtual Slide Normal Smear (Web viewer) Virtual Slide Patient Smear (Web viewer)
CASE 1: A 19-year-old woman with anemia presents with a two day history of fever and joint pain. She reports experiencing similar episodes 2-3 times/year that respond to hydration and pain medication. Her history is notable for avascular necrosis of the left femoral head at age 14. What are the major RBC abnormalities on the smear ? Many sickle cells and some polychromasia (young RBCs; nucleic acid stains blue, protein red with Wright stain). Marked variability in red cell shape (poikilocytosis), a few target cells and occasional RBC with small, dark blue inclusions (Howell-Jolly bodies, nuclear fragments) indicate splenic hypofunction from repeated infarcts(“autosplenectomy”). Occasional activated lymphs (? viral infection triggered sickle crisis). A diagnosis of the "process" is readily made by inspection of the smear. What additional test(s) establish etiology? A patient with multiple sickle crises/year is likely to have a moderate-severe form of the disease and, most likely, would have been diagnosed in infancy or childhood. Hemoglobin electrophoresis establishes a diagnosis in most cases. What would you expect the red cell indices to show in this case ? Generally normochromic and normocytic. If you just had the CBC and red blood cell indices, what other types of anemia would you consider ? Differential diagnosis of a normochromic, normocytic anemia includes decreased red blood cell production (e.g., aplastic anemia, some cases of anemia of chronic disease), acute (uncompensated) blood loss, other hemolytic anemias. How do the abnormal RBC produce symptoms, signs and complications in this disease ? Sickled cells are stickier and stiffer than normal RBCs thus "adhere" to endothelium, to one another and to WBCs, particularly in post-capillary venules, producing thrombosis. During "painful crises" (triggered by hypoxia, infection), sickled fraction increases resulting in thromboses in many microvascular beds. Ischemia and infarction ensues with cumulative organ damage in multiple organs.
CASE 2: The patient is a 28-year-old woman in the second trimester of pregnancy. Her pregnancy has been uncomplicated but she tires easily and gets short of breath with exertion. She reports episodes of light-headedness, though not to the point of fainting. Patient has tachycardia at rest, pale gums and nail beds. Normal smear stack Patient stack Virtual Slide Normal Smear (Web viewer) Virtual Slide Patient Smear (Web viewer)
CASE 2: The patient is a 28-year-old woman in the second trimester of pregnancy. Her pregnancy has been uncomplicated but she tires easily and gets short of breath with exertion. She reports episodes of light-headedness, though not to the point of fainting. Patient has tachycardia at rest, pale gums and nail beds. What are the major RBC abnormalities on the smear ? Hypochromia, anisocytosis, microcytosis and poikilocytosis. A diagnosis of the "process" is readily made by inspection of the smear. What additional test(s) establish etiology? Serum ferritin, iron and iron-binding capacity to confirm iron deficiency anemia (IDA). If IDA confirmed still need to establish cause. Insufficient intake most common cause in healthy pregnant women but want to rule out occult blood loss. What would you expect the red cell indices to show in this case ? Hypochromic, microcytic anemia. If you just had the CBC and red blood cell indices, what other types of anemia would you consider ? Differential diagnosis of microcytic, hypochromic anemia includes iron deficiency, thalassemias, anemia of chronic disease/inflammation, and lead poisoning. How do the morphologic and biochemical abnormalities produce symptoms, signs and complications in this disease ? Reduced oxygen carrying capacity. Fatigue, tachycardia, shortness of breath, pale gums and nail beds. Occasionally, bizarre appetites for substances that are largely non-nutritive (e.g., clay, soil, sand, paper, ice), termed pica.
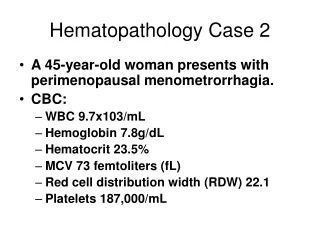
CASE 3: A 50-year-old woman with a history of Type II diabetes mellitus, hypertension, and chronic obstructive pulmonary disease felt well until 4 days prior to hospitalization when she developed crampy abdominal pain and deteriorating mental status. There was no prior history of a hematologic disorder. Normal smear stack Patient stack
CASE 3: A 50-year-old woman with a history of Type II diabetes mellitus, hypertension, and chronic obstructive pulmonary disease felt well until 4 days prior to hospitalization when she developed crampy abdominal pain and deteriorating mental status. There was no prior history of a hematologic disorder. What are the major RBC abnormalities on the smear? Substantial poikilocytosis including many schistocytes, occasional spherocytes, and some polychromasia. This constellation of microangiopathic features was found in the context of profound thrombocytopenia. A diagnosis of the “process” is readily made by inspection of the smear. What additional tests may help to confirm the morphologic impression and subclassify this process? Measurements of serum lactate dehydrogenase (LDH), unconjugated bilirubin, and haptoglobin help to confirm the impression of microangiopathic hemolytic anemia (MAHA). Screening coagulation assays (e.g., prothrombin time, activated partial thromboplastin time) and other tests (e.g., ADAMTS13 level) can help to refine the diagnosis (e.g., discriminate disseminated intravascular coagulation (DIC) from thrombotic thrombocytopenic purpura (TTP)). What would you expect the red cell indices to show in this case? Generally normocytic and normochromic. What is the physical basis for the observed red cell morphology? Shear stress or mechanical trauma disrupts the red cell membrane, resulting in formation of red cell fragments (schistocytes and microspherocytes). There is laboratory evidence of intravascular hemolysis as red cells are damaged by contact with fibrin/platelet aggregates. The polychromasia reflects compensatory reticulocytosis. Disorders commonly associated with fragmentation hemolysis include DIC, TTP, and hemolytic uremic syndrome (HUS). Prosthetic cardiac valves and areas of highly turbulent flow (e.g., severe aortic stenosis) sometimes cause shear stress on red cells resulting in schistocyte formation.
SUMMARY AND REVIEWMECHANISTIC CLASSIFICATION OF ANEMIA • Blood Loss Examples: - Acute – trauma; surgery - Chronic – lesions of GI or GU tracts II. Increased RBC destruction (hemolytic anemias) Examples: - Hereditary – hemoglobinopathies; RBC membrane or enzymatic defects - Acquired – autoimmune hemolysis; mechanical trauma to red cells • Impaired RBC production Examples: - Aplastic anemia - Defective DNA synthesis (B12/folate) - Defective heme synthesis (iron) REMEMBER THE UTILITY OF THE RETICULOCYTE COUNT IN DISCRIMINATING THESE CATEGORIES !
SUMMARY AND REVIEWCLASSIFICATION OF ANEMIA ACCORDING TO MEAN CELL VOLUME (MCV) • MICROCYTIC Examples: iron deficiency; thalassemia; some cases of anemia of chronic disease/chronic inflammation II. NORMOCYTIC Examples: sickle cell anemia; hereditary spherocytosis; some cases of anemia of chronic disease/chronic inflammation; some cases of hemolytic anemia • MACROCYTIC Examples: vitamin B12 or folic acid deficiency (megaloblastic anemias); liver disease; hypothyroidism; some cases of hemolytic anemia (e.g., those with a particularly prominent reticulocytosis; reticulocytes are slightly larger than more mature red cells, on average, and will raise the MCV)