Download
1 / 39
390 likes | 430 Views
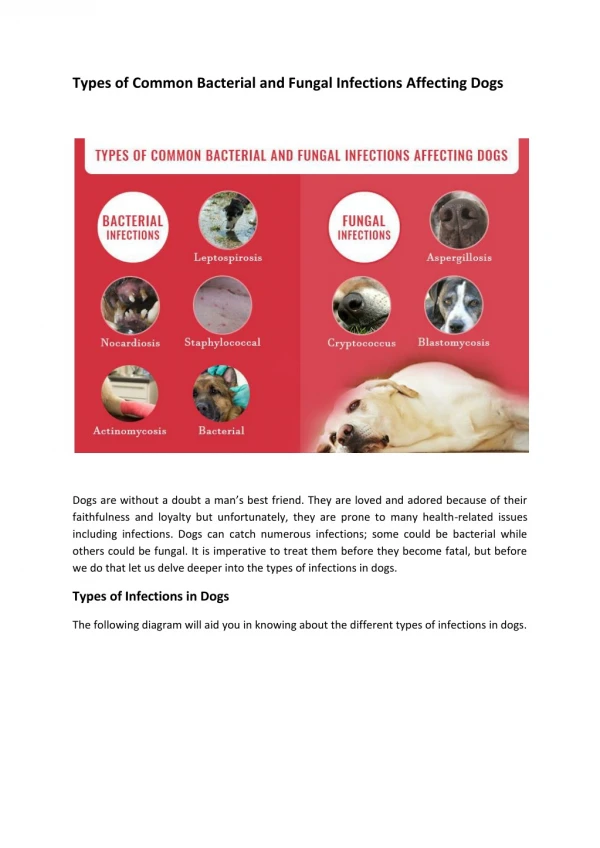
Bacterial and fungal infectious diseases, affecting the oral mucosa. Acute disease from the group of respiratory infections which characterized by fibrinous inflammation of muco u s membranes of oral cavity, nasopharynx, larynx with toxic lesion of cardiovascular and nervous systems.

E N D
Bacterial and fungal infectious diseases, affecting the oral mucosa
Acute disease from the group of respiratory infections which characterized by fibrinous inflammation of mucous membranes of oralcavity, nasopharynx, larynx with toxic lesion of cardiovascular and nervous systems
Etiology Corynebacterium diphtheriae (Leffler rod) • Grampositive, nonmotile • Don’t forms spores and capsules • ColouredbyNeisser in brown-yellow color • Ru, Leffler, Claubergmediums - blood agar with tellurium salts • Cultural-biochemical types of C.diphtheriae - mitis, gravis, intermedius • Production of very strong exotoxin (gene tox +) • Structure of exotocin - dermanecrotoxin, hemolysin, neuraminidase, hyaluronidase • Firm to low temperature, long save on a dry surfaces; high responsive to heating and desinfection solutions
Epidemiology • Source – sick person or carrier (convalescent or health) of toxicogenic strains • Ways of transmission - airborne, contact - household (occasionally) • Sensibility is high, adultsmore often become sick (80 %) • Case rate sporadic, outbreaks are possible • Immunodefence antitoxic, postvaccine • Seasonal character - autumn - winter
Diphtheria cases reported to World Health Organization between 1997 and 2007
Pathogenesis • Penetration of the agent through entrance gate (mucous of upper respiratory tract, sometimes conjunctivas, skin) • Production of exotoxin • Local and systemic effects of the toxin: • Dermonecrotoxin - necrosis of a surface epithelium, retardation of blood stream, rising of a permeability of vessels, their fragility, transuding of plasma in ambient tissues, formation of a fibrinous film, edema of tissues; downstroke of pain sensitivity
Pathogenesis • Neuraminidase - replacement of cytochrome, blockage of cellular respiration, destruction of a cell, violation of a function of organs and tissues (central and peripheric nervous system, cardiovascular system, kidneys) • Hyaluronidase - destruction of a stroma of a connecting tissue (rising of permeability of vessels, edema of tissues) • Hemolysin - hemorrhagic set of symptoms
Clinical manifestation • Incubation period – 2-10 days • Phenomena of intoxication (high fever, malaise, general weakness, headache) • Pharyngalgia - moderate • Changes of a throat mucous - soft hyperemia, edema of tonsills, covers on their surface (grey colour, dense, hard to remove with bleeding, slime), spread out of tonsills limits(palatopharyngeal arches, uvula, soft palate) • Augmentation and moderate morbidness of regional lymphnodes • Edema of a hypodermic fat of a neck
Peculiarities of diphtheria covers (Grey colour, dense, hard to remove with bleeding, slime), spread out of tonsills limits(on uvula, soft palate, palatopharyngeal archs)
Features of diphtheria toxicosis (In wide-spread, combined, hypertoxical, hemorrhagic forms)toxicosis І, ІІ, ІІІ • Edema of the neck hypodermic tissues • Paleness of skin • Cyanosis of lips • Decreasing of arterial pressure • Tachycardia • Decreasing of a body temperature
Diphtheria of larynx Real croup (stenosis of a larynx) • І degree (catarrhal) - labored inspiration, retraction of intercostal spaces, rasping “dog barking" cough, “horse” voice • ІІ degree (stenosis) - noisy respiration, inspiratory dyspnea with an elongated inspiration, participation in respiration of auxiliary muscles, aphonia • ІІІ degree (asphyxia) - acute oxygen insufficiency, sleepiness, cyanosis, cold sweat, cramps, paradoxical sphygmus
Complications • Infectious-toxic shock • Intra vessels disseminated syndrome • Myocarditis (early, late) • Polyradiculoneuritis (early, late) • Nephrosonephritis etc.
LABORATORY DIAGNOSTIC • Detection of the agent in smears from a throat and nose (taking of material on border between effected area and normal mucous) • Microscopy (colouring byNeisser) – typical locating of rods, grains of volutin in bacterias • Sowing on convolute serum or telluric blood agar for allocation of clean culture and recognizing oftoxigenisity • Serological tests mirror a condition of immune defence (efficiency of vaccination)
Treatment • Immediate hospitalization • Bed regimen (at localized forms - 10 days, at toxic - not less than 35-45 days) • Specific treatment - introducing of antitoxic antidiphtherial Serum (from 30-50 thousand IU at the localized forms up to 100-120 thousand IU at toxic, byBezredka method) • Glucocorticoids (in toxic forms and croup) • Antibiotics (penicilini, tetracyclini, erythromycini) • Strychninum (in toxic forms) • In case of croup - inhalations, broncholitics, diuretics, glucocorticoids, antibiotics, antihistamine, lytic admixture; under the indications - intubation, tracheotomy
Conditions of discharging from a hospital • Clinical convalescence • 2 negative results of bacteriological research of smears from a throat and a nose with two-day interval • For decret group - additional doublebacteriological examination in polyclinic
Prophylaxis • Plan immunization(vaccination in 3, 4, 5 months.With АPДT vaccine, revaccination in 18 months; 6, 11, 14, 18 yearsand adults every 10 yearswith АДT-М vaccine) • In the focus – 7 daysmedical observation after contact persons Bacteriological examination Sanation of detected carriers Final disinfection Revaccination
Desinfection • Aeration and ultra-violet lighting of puttings, wet cleaning with usage of 2/3-basic salt of perchloron, calcium of hypochlorite, 3 % of solution of chloraminum, 1 % of solution amfolan • Sputum, the outwashes from a nasopharynx hash with double quantity of solutions, exposition 2 hours. The tableware is boiled in 2 % potassium solution 30 mines. Bed-clothes and clothes if necessaryto decontaminate in desinfection camera
Differential diagnosis • Tonsillitis, including Plaut-Vincent-Simanovsky • Herpetic tonsillitis • ARVI (adenoviral infection, false croup) • Paratonsillar abscess • Infectious mononucleosis • Scarlet fever • Pseudotuberculosis • Tonsillo-bubonic form of tularemia • Mycotic affection of tonsills • Epidemic parotitis • Typhoid fever • Lues • Hematological diseases (acute leukosis, agranulocytosis)
Acute infection of respiratory tract, which is caused by meningococcous (Neisseria meningitidis) and clinically represents in the forms of nasopharyngitis, sepsis or meningitis
The source of disease: • carriers (1 case per 2000 carriers) • patients with meningococcal nasopharyngitis • patients with generalized forms of infection
Mechanism of transmission – air-drop Seasonal occurrence – February-April Most of the patients are children under 10 Morbidity is sporadic, sometimes epidemic Immunity is type-specific, steady
Classification: I. Primarily localized forms: - meningococcal carrier state; - acute nasopharyngitis; II. Hematogenic generalized forms: - meningococcemia; - meningitis; - meningoencephalitis; III. Mixed forms (meningococcemia+meningitis); IV. Rare forms (endocarditis, arthritis, irideocyclitis, pneumonia). Complications: severe brain edema, infectious-toxic shock
Rashes peculiarities: • haemorrhagic; • localization on buttocks, thighs, shins, trunk; • a lot of elements; • different sizes of elements – from patechial to the spread hemorrhages; • non correct form, often star-like; • different coloring and brightness of elements; • necrosis in place of considerable hemorrhages with formation of defects; • often combination of hemorrhages with roseolla and papules.
Laboratory diagnostics 1. Revealing of infectious agent in smears from pharynx, blood, liquor - the material for stain should be taken without touching of mucous membrane of cheeks and tongue. Microscopy: gram-negative diplococci with intracellular localization 2. Serologic tests: in dynamic with interval 5-7 days 3. Express-diagnosis: immunofluorescent method.
Treatment Generalized forms: • immediate hospitalization • antibiotics in large doses (benzylpenicilline 200 000 – 500 000 U/kg, levomycetini succinatis) • corticosteroids • dehydratation therapy (in case of meningitis) • desintoxication • treatment of disseminated intravessel coagulation (heparin, contrical, human plasma) Sanation of meningococcus carriers: • antibiotics in common doses (ampicillini, levomycetini, rifampicini) • local sanation (ultraviolet, ultrasonic) • desensibilisation therapy
HIV-Infection - viral disease of human, which is passed mainly by sexual and parenteral ways and characterized by long-term persistence. Defeat of the thymus gland’s system of immunity, causes clinically expressed form – syndrome of acquired immune deficiency (AIDS) with lymphadenopathy, intoxication, spreading of infectious diseases and oncological processes
Properties of Kaposhi sarcoma in patients with AIDS: - strike the persons of age young and middle - primary elements appear on a head and trunk - become purulent and varicosity - metastasizes in internal organs, has a malignant course - is marked by high lethality, patients more frequent does not exceed 1,5 year