
Cardiovascular/Circulatory System
Cardiovascular/Circulatory System. CHAPTER 12- & 13. Intro Cardiovascular/Circulatory System. Functions to transport oxygen, nutrients, cell wastes, & hormones via the blood Intro to Cardiovascular System ● Blood alternates between 2 circuits

Cardiovascular/Circulatory System
E N D
Presentation Transcript
Cardiovascular/Circulatory System CHAPTER 12- & 13
Intro Cardiovascular/Circulatory System Functions to transport oxygen, nutrients, cell wastes, & hormones via the blood Intro to Cardiovascular System ● Blood alternates between 2 circuits - Pulmonary Circuit – carries blood from heart to lungs where blood is oxygenized and then carries it back to the heart - Systemic Circuit – carries blood from heart to the body and then back to the heart
Intro Cardiovascular/Circulatory System Intro to Cardiovascular System ● 3 Types of Blood Vessels - Arteries– carry blood away from the heart - Veins– carry blood to the heart - Capillaries – network of small blood vessels between arteries and veins that exchange materials between blood and tissues http://www.youtube.com/watch?v=GbttJ-5do9M&feature=related
12-1 The Heart - Anatomy The Heart • Location and size: approx. size of a person’s fist • Enclosed within the mediastinum, the middle cavity of the thorax, intermediate to the lungs • Its pointed apex is directed toward the left, rests on the diaphragm, at about the fifth intercostals space • Its base points toward the right shoulder and lies beneath the second rib (great vessels emerge from here)
12-1 The Heart - Anatomy • Coverings and wall • Enclosed by a double sac of serous membrane, called the pericardium • thin epicardium, or visceral pericardium, tightly hugs the external surface of the heart and is part of the heart wall. • Is continuous at the base with the loose parietal pericardium, which is reinforced on its superficial face by dense connective tissue, known as the fibrous pericardium; helps protect the heart and anchors it to surrounding structures, such as the sternum and diaphragm • A slippery lubricating fluid, pericardial fluid is produced so the heart beats in a frictionless environment
12-1 The Heart - Anatomy • Coverings and wall • Walls of the heart composed of three layers: • 1. epicardium – (outer layer) is the visceral pericardium; • 2. myocardium – (middle layer) thick bundles of cardiac muscle twisted and whorled into ring-like arrangement • layer that actual contracts • is reinforced internally by a dense, fibrous connective tissue network – “skeleton of the heart” • 3. endocardium – (innermost layer) squamous endothelium that lines the chambers • is continuous with the blood vessels leaving and entering the heart
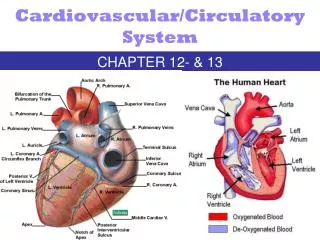
12-1 The Heart - Anatomy • Chambers and associated great vessels • Four hollow chambers: • 2 atria – receiving chambers divided by interatrial septum • blood flows into the right atrium under low pressure from the veins of the body and then fills the right ventricle • Blood flows into the left atrium from the pulmonary veins of the lungs • 2 ventricles – discharging chambers divided by the interventricular septum • pumps the heart – when they contract, blood is propelled out of the right ventricle to the lungs and out of the left ventricle into the circulation of the body • Coronary sulcus divides atria from ventricles
12-1 The Heart - Anatomy • Great vessels • Superior and Inferior vena cava receives relatively oxygen-poor blood from the systemic veins of the body into the right atrium of the heart • Pulmonary trunk takes the oxygen-poor blood from the right ventricle to the pulmonary arteries • Right & Left Pulmonary arteries split out from the pulmonary trunk and carry oxygen-poor blood to the lungs where O2 is picked up and CO2 is unloaded • 2 Right & 2 Left Pulmonary veins return the now oxygenated blood from the lungs to the left atrium of the heart • Aorta takes the oxygenated blood from the left ventricle out to the systemic arteries • ***Because the left ventricle supply the blood for the entire body, the muscles are much thicker
12-1 The Heart - Anatomy • Valves: 4 • Atrioventricular Valves (AV)- located between atria and ventricles; prevent backflow into the atria when the ventricles contract • 1. bicuspid, or mitralvalve- left side (2 flaps of endocardium) • 2. tricuspid valve- right side (3 flaps) • chordae tendinae – “heart strings”; anchor flaps to the walls of the ventricles (papillary muscles); so during contraction, when pressure builds, and flaps close, they don’t flip ‘backwards’ into the atria
12-1 The Heart - Anatomy • Valves: 4 • Semilunar Valves – guards the bases of the two large arteries leaving the ventricular chambers; each valve has 3 leaflets that fit tightly together when closed; when ventricles contract and force blood out of the heart, the leaflets are forced open & flattened against the walls of the arteries; when ventricles relax, blood flows backward toward the heart, and the leaflets fill with blood, closing the valves • 3. pulmonary semilunar valve – between rt. ventricle and pulmonary trunk • 4. aortic semilunar valve – between left ventricle and aorta
12-1 The Heart - Anatomy • Valves: 4 • Valve Disorders • Heart murmur – backflow of blood into the atrium when ventricle contracts • Mitral valve prolapse – cusps of the valve do not close completely • Transcatheter Aortic Valve Replacement Surgery • Open Heart Aortic Valve Replacement • Minamally Invasive Aortic Valve Replacement
12-1 The Heart - Anatomy • Coronary circulation • The blood supply that oxygenates and nourishes the heart tissue is provided by the right and left coronary arteries, which further branch into smaller arteries; if any of these become constricted or clogged, can result in a myocardial infarction (MI)- death to the myocardial cells; AKA. heart attack or coronary • Great cardiac vein and other veins take waste material away from heart tissue
12-1 The Heart - Anatomy Systemic Circulation CARDIAC CIRCULATION – path of blood flow 1. superior & inferior vena cava (O2 poor blood enters the heart) 2. right atrium 3. tricuspid valve 4. right ventricle 5. pulmonary semilunar valve 6. right & left pulmonary arteries via pulmonary trunk (rt & lft lungs) 7. lungs – gas exchange (blood becomes oxygenated) 8. O2 rich blood returns to heart through 4 pulmonary veins (2 right, 2 left) 9. enters left atrium 10. bicuspid valve 11. left ventricle 12. aortic semilunar valve 13. Aorta 14. to the body (systemic circulation) http://www.youtube.com/watch?v=mDSFxcf2UgQ Pulmonary Circulation Systemic Circulation
12-2 The Heartbeat - Physiology • 2 Types of Cardiac Muscle Cells • Contractile cells – similar to skeletal muscle cells, create contractions to propel blood • Action potential similar to skeletal, but the cardiac cells contract about 25x longer • Conducting cells – mix between nervous and muscle cells can conduct contraction stimulus– nodal cells establish rate of cardiac contractions
12-2 The Heartbeat - Physiology • Intrinsic conduction system of the heart: Setting the basic rhythm • Unlike skeletal muscle cells that need a nerve impulse to stimulate them to contract, cardiac cells contract spontaneously and independently; atrial cells- 60x/min and ventricle cells- 20-40x/min • Two systems act to regulate heart activity: • 1. Autonomic nervous system can speed up and slow down the heart rate • 2. Intrinsic conduction system, or nodal system - is built into the heart tissue and sets its basic rhythm; causes heart muscle to depolarize in only one direction-from the atria to ventricles; enforces a contraction rate of about 75 bpm
12-2 The Heartbeat - Physiology • Intrinsic conduction system of the heart • 2. Intrinsic conduction system, or nodal system • Sinoatrial (SA) node - located in right atrium; “pacemaker of the heart”; starts each heartbeat and sets the pace of the heart (70-80 action potentials/min.); from SA node, impulse spreads through atria to the: • Atrioventricular (AV) node - at junction of atria and ventricles; atria contract together; impulse is delayed briefly to give the atria time to finish contracting (40-60 action potentials/min.), it then passes rapidly through the:
12-2 The Heartbeat - Physiology • 2. Intrinsic conduction system, or nodal system (cont.) • Atrioventricular (AV) Bundle (Bundle of his) • Bundle branches - right and left; located in interventricular septum • Purkinje fibers - spread within the muscle of the ventricle walls • causes a “wringing” contraction of the ventricles that begins at the heart apex and moves toward the atria; this contraction effectively ejects blood superiorly into the large arteries leaving the heart.
12-2 The Heartbeat - Physiology • Problems: • Fibrillation – rapid, uncoordinated shuddering of the heart; makes heart totally useless as a pump; is major cause of death from MI • AED can be used in emergencies to bring heart back into normal rhythm. To be used in conjunction with CPR (“Stayin’ Alive” is rhythm for compressions) • Tachycardia – rapid heart rate (>100bpm); if prolonged, may progress to fibrillation • Bradycardia – slower than normal heart rate (<60bpm)
12-2 The Heartbeat - Physiology • Electrocardiogram (ECG/EKG) - recording of electrical impulses, traces flow of current through heart; typically has 3 waves: • P wave- small; signals depolarization of atria immediately before they contract • QRS wave- large; results from the depolarization of ventricles, precedes ventricular contraction • T wave-repol. of ventricles (atrial repol. is hidden by QRS wave) Cardiac arrythmia– abnormal pattern of cardiac activity, not inherently dangerous but can lead to problems
12-3 The Heart – Cardiac Cycle • Cardiac cycle and heart sounds • Cardiac Cycle – refers to events of one complete heartbeat, during which both atria and ventricles contract and then relax (about 0.8 seconds); when heart rate increases, phases are shortened, especially diastole • Systole – contraction of ventricles; atria are relaxed and filling up with blood , blood pressure (BP) rises • Diastole – relaxation of ventricles; blood is flowing into and through the atria into the ventricles from the pulmonary and systemic circulations, then atria contract and force the blood remaining in their chambers into the ventricles, BP falls • Lubb – Dupp - heart sound; “lubb”- noisy turbulence heard when the blood hits the AV valves after they close; “dupp”- noisy turbulence heard when the blood hits the SL valves after they close • 2 softer sounds caused by blood flowing into ventricles when atria contract
12-3 The Heart – Cardiac Cycle • Cardiac cycle and heart sounds (pg. 357)
12-4 The Heart – Cardiac Output • Cardiac output (CO) • amount of blood pumped out by each ventricle in 1 minute; is product of heart rate (HR) in beats per minute (bpm) and stroke volume (SV)- amount of blood pumped out by a ventricle with each heartbeat - in ml per minute (ml/min) • CO= HR X SV= ml/min • Average CO = 75bpm x 70ml/beat = 5250 ml/min • since normal adult blood volume is about 5000 ml, the entire blood supply passes through the body once each minute • Regulation of stroke volume- Starling’s Law of the Heart- the critical factor controlling stroke volume is how much the cardiac muscle cells are stretched (by venous return) just before they contract; the more they are stretched, the stronger the contraction will be; anything that increases the volume or speed of venous return also increases stroke volume and force of contraction (atrial or Bainbridge reflex)
12-4 The Heart – Cardiac Output • Cardiac output (CO) • Factors modifying basic heart rate • Neural (ANS) controls- during times of physical or emotional stress, the sympathetic nervous system stimulates the SA node, AV node, and cardiac muscle; parasympathetic nervous system slows it down after a stress response; various hormones (epinephrine and thyroxine) and ions (Ca2+, Na+, K+) can have an effect • Physical factors- ex. age (fastest in fetus-140-160bpm), gender (females: 72-80bpm & males: 64-72bpm), exercise (faster), and body temperature (higher temperature=faster) can influence heart rate
Diseases of the Heart • Congestive Heart Failure (CHF)- when the pumping efficiency of the heart is depressed so that circulation is inadequate to meet tissue needs; failure of one side of the heart puts a greater strain on the opposite side, and eventually the whole heart fails • pulmonary congestion - when the left side of the heart fails, the right side keeps pumping to the lungs, but the left side is unable to eject the returning blood into the systemic circulation; as blood vessels within the lungs become swollen with blood, the pressure within them increases, and fluid leaks from the circulation into the lung tissue causing pulmonary edema; if untreated, the person suffocates • peripheral congestion - occurs as blood backs up in the systemic circulation; edema is most noticeable in the distal parts of the body which become swollen and puffy
13-1 Blood Vessels MICROSCOPIC ANATOMY OF BLOOD VESSELS • Tunics • Tunica intima - lines the lumen or interior of the vessels; is a thin layer of endothelium (squamous epithelial cells) resting on a basement membrane; cells fit closely together to form a slick, frictionless surface • Tunica media - bulky middle layer; mostly smooth muscle controlled by the sympathetic nervous system for vasodilation (muscles relax, diameter increases) or vasoconstriction (muscles contract, diameter decreases) and elastic tissue • Tunica externa - the outermost layer; largely fibrous ct. tissue; supports and protects vessels • A vascular shunt - a vessel that directly connects the terminal arteriole and postcapillaryvenule at opposite ends of the bed • True capillaries - the actual exchanging vessels; a precapillary sphincter surrounds the root of each true capillary and acts as a valve to regulate flow of blood into the capillary
13-1 Blood Vessels MICROSCOPIC ANATOMY OF BLOOD VESSELS • Structural differences between vessels • Arteries- walls, especially tunica media, thicker than veins; needs to expand and recoil • Veins- low pressure, so walls tend to be thinner; larger lumen with valves to prevent backflow
13-1 Blood Vessels MICROSCOPIC ANATOMY OF BLOOD VESSELS • Structural differences between vessels (cont.) • Veins- • muscular pump- when skeletal muscles contract, they squeeze nearby veins • respiratory pump- when we inhale, the drop in pressure in the thorax causes the large veins near the heart to expand and fill, helping blood return to the heart • Varicose veins/hemorrhoid- valves break; vein becomes twisted and dilated
13-1 Blood Vessels MICROSCOPIC ANATOMY OF BLOOD VESSELS • Structural differences between vessels (cont.) • Capillaries- only a tunica intima; therefore exchange occurs here; capillaries form interweaving networks called capillary beds - consist of two types of vessels: • A vascular shunt - a vessel that directly connects the terminal arteriole and postcapillary venule at opposite ends of the bed • True capillaries - the actual exchanging vessels; a precapillary sphincter surrounds the root of each true capillary and acts as a valve to regulate flow of blood into the capillary
13-1 Blood Vessels Diseases of the Blood Vessels • Arteriosclerosis – a thickening and toughening of the arterial walls • Focal Calcification – degenerating smooth muscle in tunica media replaced by calcium deposits • Atherosclerosis – formation of lipid deposits in tunica media that eventually triggers the creation of plaque – a fatty mass of tissue projecting from the lumen • Known as the “silent killer”
13-2 Physiology of Circulation • Arterial Pulse • Pulse - a pressure wave that travels through the entire arterial system due to the alternating expansion and recoil of an artery that occurs with each beat of the left ventricle; influenced by activity, postural changes, and emotions • also called pressure points because they are compressed to stop blood flow into distal tissues during hemorrhage • compress artery firmly as you begin and then immediately ease up on your pressure slightly; notice the regularity of the pulse and its relative strength Vital Signs – pulse, blood pressure, respiratory rate, body temperature
13-2 Blood Pressure • Blood Pressure - the pressure the blood exerts against the inner walls of the blood vessels; is the force that keeps blood circulating continuously even between heartbeats; unless stated otherwise, means the pressure within the large systemic arteries near the heart • Blood pressure gradient- highest in large arteries coming off of the heart, decrease until get to the venae cavae, where pressure is zero or even negative; it’s the arteries recoiling ability that keeps pressure on blood • Measuring blood pressure • Systolic pressure- pressure in arteries at peak of ventricular contraction • Diastolic pressure- pressure when the ventricles are relaxing • Reported in mmHG; systolic/diastolic; measured indirectly by the auscultatory method - using a sphygmomanometer and a stethoscope to auscultate (listen): • the first “lubbdupp” you hear = systolic rate • the last “lubbdupp” you hear = diastolic rate • The sounds are known as the “sounds of Korotkoff” • How to take manual BP
13-2 Blood Pressure • Effects of various factors on blood pressure • BP= CO X PR (peripheral resistance)- the amount of friction encountered by the blood as it flows through the blood vessels • affected by many factors: • diameter of blood vessels (constriction ↑BP, dilation ↓BP) • blood volume • blood viscosity • any factor that increases either the CO or PR causes an almost immediate reflex rise in blood pressure • age • weight • time of day • exercise • body position • emotional state • various drugs, etc.
13-3 Effects on Blood Pressure • Effects of various factors on blood pressure • Neural factors: the autonomic nervous system- • Sympathetic nervous system causes vasoconstriction, or narrowing of blood vessels, when: • (1) you’re lying down and quick stand up, baroreceptors (pressoreceptors) in large arteries of neck and chest are activated by the low blood pressure, cause vasoconstriction to increase BP • (2) during hemorrhage, due to decrease pressure, the heart beats more rapidly, vasoconstriction occurs to bring blood pressure back up • (3) we’re frightened, stressed, etc., sympathetic nervous system causes a generalized vasoconstriction, except in the skeletal muscles, which vasodilate to increase blood flow for “fight or flight” (note: sympathetic nerves never cause vasoconstriction of the heart or brain blood vessels)
13-3 Effects on Blood Pressure • Effects of various factors on blood pressure • Renal factors: the kidneys- play a role in BP by altering BV (blood volume): • If BV or BP is higher then normal, kidneys allow more water to leave the body in the urine, decreasing BV, thus decreasing BP and vice versa • Also, when BP is low, kidney cells release renin, an enzyme that results in the formation of angiotensin II, a potent vasoconstrictor, and stimulator of adrenal cortex to release aldosterone, a hormone that enhances sodium reabsorption by the kidneys; as sodium moves into the blood, water follows, increasing blood volume, increasing blood pressure
13-3 Effects on Blood Pressure • Effects of various factors on blood pressure • Endocrine factors: various hormones affect blood pressure • Epinephrine & Norepinephrine ↑CO and ↑BP • Antidiuretic Hormone ↑blood volume and vasoconstriction • Erythropoietin ↑blood volume
13-4 Shock • Variations in blood pressure • Hypotension- low blood pressure (systolic < 100mmHg) • Hypertension- high blood pressure (systolic > 140 mmHg) • Shock – acute circulatory crisis marked by low BP and inadequate peripheral blood flow • Symptoms: • Hypotension with systolic below 90mmHg • Pale, cool, moist (clammy) skin due to peripheral vasoconstriction and sympathetic activation of sweat glands • Confusion and disorientation due to decrease BP in brain • Rise in heart rate & rapid, weak pulse • Reduced blood flow stops urine production • Drop in blood pH due to lactic acid build-up in O2 deprived cells
13-5 & 13-6 Pulmonary Circuit & Systemic Circuits • Pulmonary and Systemic Circuits review • Pulmonary Circuit • Pulmonary trunk, right & left pulmonary arteries carry deoxygenated blood from heart to lungs • 4 pulmonary veins carry oxygenated blood from lungs to heart
Ascending aorta R & L coronary aa. Aortic arch Brachiocephalic a. R. common carotid a. R. subclavian a. L. common carotid a. L. internal carotid a. L. external carotid a. L. subclavian a. Vertebral a. Becomes the axillary a. in the axilla And then continues in the arm as the brachial a. Radial a. Ulnar a. Thoracic aorta (not illustrated in textbook) Intercostals aa. Bronchial aa. Esophageal aa. Phrenic aa. 13-7 Gross Anatomy of Blood Vessels MAJOR ARTERIES OF SYSTEMIC CIRCULATION
Abdominal aorta Celiac trunk L. gastric a. Splenic a. Common hepatic a. Superior mesenteric a. Renal aa. (R. & L.) Gonadal aa. (R. & L.) Ovarian aa. Testicular aa. Lumbar aa. (not pictured in textbook) Inferior mesenteric a. Abdominal Aorta (cont.) Common iliac aa. (R. & L.)- each branches into: Internal iliac a. External iliac a.- enters the thigh and becomes the femoral a.- branches into the: Deep femoral a. Femoral a. becomes popliteal a. at knee Splits into anterior and posterior tibial a., which terminates in the: Dorsalis pedis a. 13-7 Gross Anatomy of Blood Vessels MAJOR ARTERIES OF SYSTEMIC CIRCULATION
Superior and inferior vena cava Veins draining into the superior vena cava Radial and ulnar vv.; unite to form brachial v. which empties into the axillary v. Cephalic v. Basilica v. Median cubital v. Subclavian v. External jugular v. Vertebral v. Internal jugular v. Brachiocephalic vv. (R. & L.) Azygos v. (not illustrated) Veins draining into the inferior vena cava Anterior and posterior tibial vv. Post. tibial v. becomes popliteal v. Femoral v. External iliac v. Fibular v. Great saphenous vv. Dorsal venous arch Common iliac vv. External and internal iliac vv. R & L gonadal v. (not illustrated) Renal vv. Hepatic portal v. R & L hepatic vv. 13-7 Gross Anatomy of Blood Vessels MAJOR VEINS OF SYSTEMIC CIRCULATION
13-7 Special Circulations • Hepatic Portal Circulation- veins of hepatic portal circulation drain the digestive organs, spleen, and pancreas and deliver this blood to the liver through the hepatic portal vein; since the liver is a key body organ involved in maintaining the proper glucose, fat, and protein concentrations in the blood, this system “takes a detour” to ensure that the liver processes these substances before they enter the systemic circulation; some nutrients are even removed to be stored or processed in various ways for later release into the blood
13-8 Special Circulations • Fetal Circulation- since lungs and digestive systems are not yet functioning, all nutrient, excretory, and gas exchanges occur through the placenta (nutrients and oxygen from mother to baby, carbon dioxide and wastes from baby to mother); mother and baby’s blood never touches • contains umbilical cord: 3 blood vessels- one large umbilical vein (carries nutrient-and oxygen-rich blood to fetus) and two smaller umbilical arteries (carries carbon dioxide and wastes from fetus to placenta) • as blood flows superiorly toward fetal heart, most blood by-passes the immature liver through the ductusvenosus and enters the inferior vena cava, which carries the blood to the right atrium of the heart
13-8 Special Circulations • Fetal Circulation (cont.) • since fetal lungs are nonfunctional and collapsed, two shunts see that they are almost entirely by-passed: some of the blood entering the right atrium is shunted directly into the left atrium through the foramen ovale - a flap-like opening in the interatrial septum (blood then goes to left ventricle where the aorta carries blood to fetal body); blood that does get into the right ventricle is pumped out the pulmonary trunk, where it meets a second shunt, the ductusarteriosus, a short vessel that connects the pulmonary trunk to the aorta • at birth, or shortly after, the foramen ovale closes, and the ductusarteriosus collapses and is converted to the fibrous ligamentumarteriosum
Special Circulations • Arterial supply of the brain and the Circle of Willis - since continual blood supply is crucial, brain supplied by two pairs of arteries (int. carotid and vertebral aa.); anterior and posterior blood supplies are united by small communicating arterial branches resulting in a complete circle of connecting blood vessels called the Circle of Willis, which surrounds the base of the brain; protects brain by providing more than 1 route for blood to reach brain tissue in case there is a clot or impaired blood flow anywhere in the system